Introduction
Before coronavirus disease 2019 (COVID-19), antimicrobial stewardship (AMS) programs were essential for managing multidrug-resistant Gram-negative bacterial infections. In contrast, antifungal stewardship (AFS) programs were uncommon as a component of AMS (1). During the COVID-19 pandemic, both AMS and AFS programs have lost their priority (2).
In a recent report, 72% (1450/2010) of the hospitalized COVID-19 patients have received antibiotics, although bacterial or fungal co-infection was detected in only 8% (62/806) of them (3). Some studies reported an increased risk of invasive fungal infections (IFI) in COVID-19 cases with comorbidities who stayed in intensive care units (ICUs) (4). The definition of COVID-19-associated pulmonary aspergillosis (CAPA) has become a new term in the medical literature (5). The diagnosis and treatment of IFI became a real challenge in the pandemic period.
In our hospital, the consultation services to patients other than COVID-19 have been delayed because of the increased workload of the infectious diseases and clinical microbiology department. The primary physicians of all patients in the wards and ICUs managed the antifungal therapy most of the time. Diagnostic laboratory tests for fungal infections were unavailable due to the increased demand for COVID-19 tests. We evaluated the effect of mandatory changes on antifungal consumption due to the pandemic and aimed to contribute to the policies for antifungal use post-pandemic period.
Materials and Methods
Grouping of Units
The study was performed in a university hospital with approximately 1000-bed, located in İzmir (Aegean Region), the third biggest city of Türkiye. The ICUs of internal medicine and anesthesia were dedicated to COVID-19 patients during the pandemic period. Non-COVID-19 ICUs included thoracic-cardiovascular surgery, neurology, coronary, and chest diseases ICUs. The sum of the antifungal consumption in these units was calculated while comparing pre-pandemic and pandemic periods.
The hematology-oncology-hematopoietic stem cell transplantation (HSCT) clinics were the least affected by the pandemic due to the physical conditions of the facility. During the pandemic, other units were grouped as medical and surgical clinics. The pandemic clinic, emergency departments, and pediatric clinics were excluded from the study.
Grouping of Drugs and the Calculation of Consumption
Our study covered the period between March-October 2019 before the pandemic and March-October 2020 during the pandemic. The data on the antifungal drug use by months and clinics were obtained from the hospital information registration system. The drugs were classified according to the World Health Organization Anatomical Therapeutic Chemical (WHO ATC) coding system, which classifies drugs according to their primary therapeutic use. Then, for each product, the daily dose (defined daily dose, DDD), which defines the unit measurement as “the average of the daily maintenance dose,” used in the main indication of the WHO in adults, was determined (6, 7). The number of beds, the occupancy rate, and the number of drug boxes consumed were obtained from the hospital information system. The antifungal consumption (DDD/100 bed-days) was calculated based on these data, and the consumption between years was compared based on clinics.
Antifungal drugs were grouped as azoles (fluconazole, voriconazole, posaconazole), echinocandins (anidulafungin, caspofungin, micafungin), and polyenes (liposomal amphotericin B).
Statistical Analysis
The data on the antifungal consumption was recorded in Microsoft Excel (Microsoft Corp., USA) with the data on the number of beds, the occupancy rate, and the number of drug boxes to calculate the number of DDD/100 bed-days. The statistical analysis was performed using the R version 4.1.3 (The R Foundation for Statistical Computing, Vienna, Austria). Differences in antifungal consumption, expressed in DDD/100 bed-days, between 2019 and 2020 were analyzed using the exact rate ratio test. For all statistical analyses, 95% CIs were calculated and p<0.05 were considered statistically significant.
Results
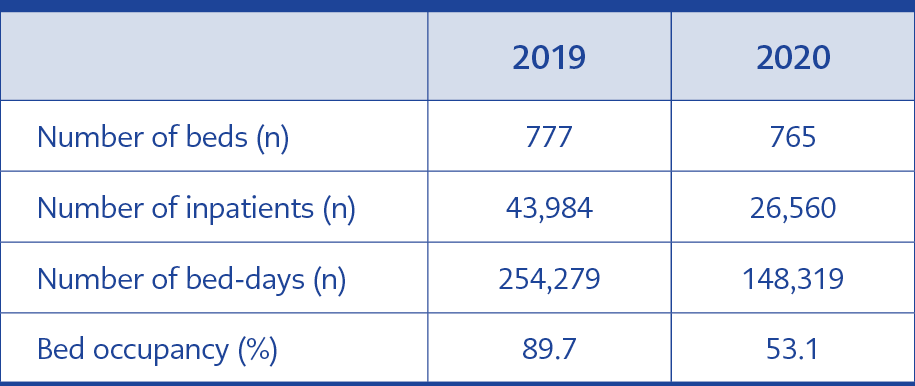
Table 1. Comparison of the number of beds, and inpatients in 2019 and 2020.
The number of inpatients, the bed occupancy rate, and the total number of bed-days significantly decreased due to the pandemic measures implemented by our hospital (Table 1).
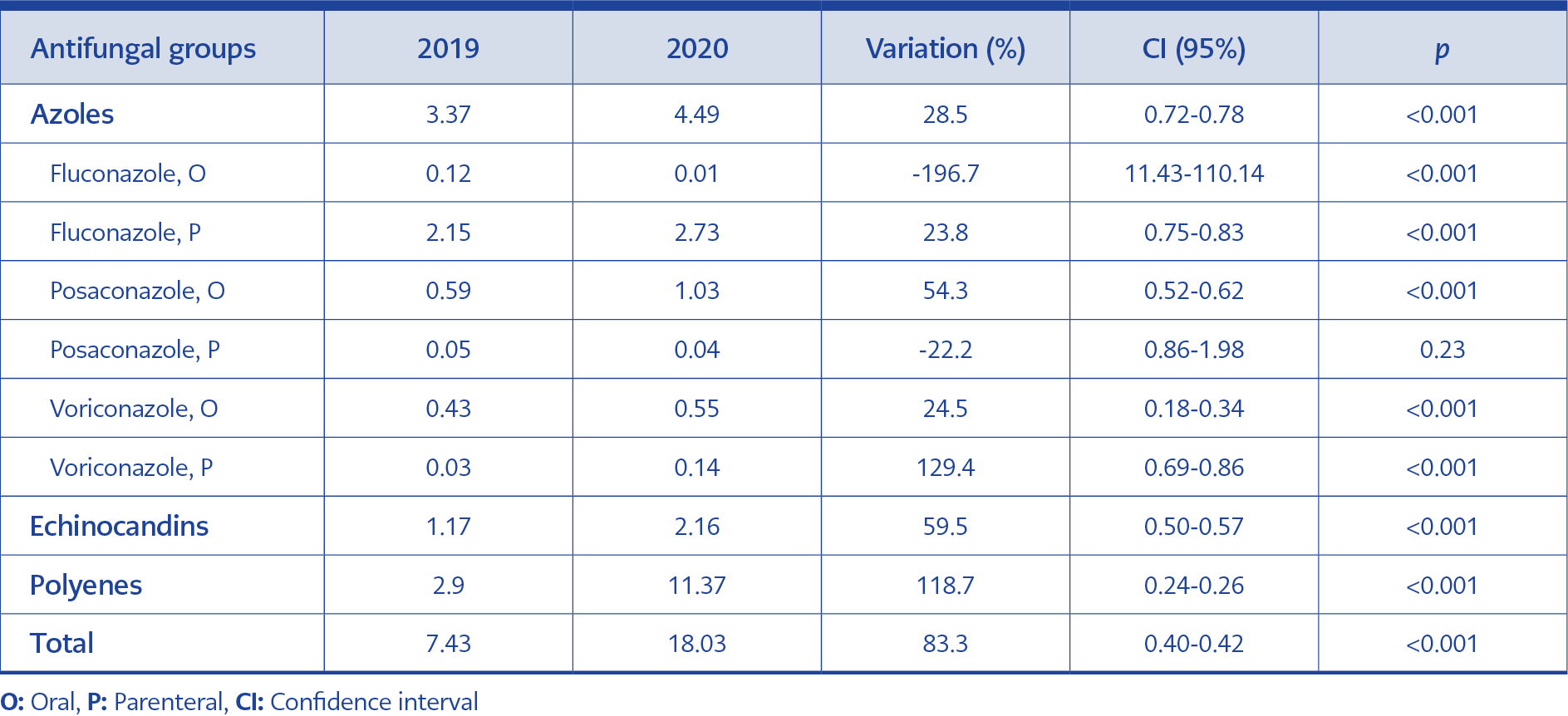
Table 2. The comparison of antifungal consumption in pre-pandemic (2019) and pandemic (2020) era (DDD/100 bed-days).
In the pandemic period, a two-fold increase (95% Cl=0.40-0.42, p<0.001) was observed in the antifungal consumption (DDD/100 bed-days), adjusted by the number of beds, occupancy rate, and the number of drug boxes consumed. A significant increase in antifungal consumption (DDD/100 bed-days) was observed in all antifungal groups; azoles (p<0.001), echinocandins (p<0.001), and polyenes (p<0.001) in the pandemic period. Polyene consumption made up the majority of this increase (Table 2). The subgroup analysis of oral or parenteral azole consumption was given in Table 2. While the consumption of oral fluconazole and parenteral posaconazole decreased, others have increased. While parenteral fluconazole was the most consumed antifungal in the azole group, the highest increase of consumption between the two periods was detected in parenteral voriconazole.
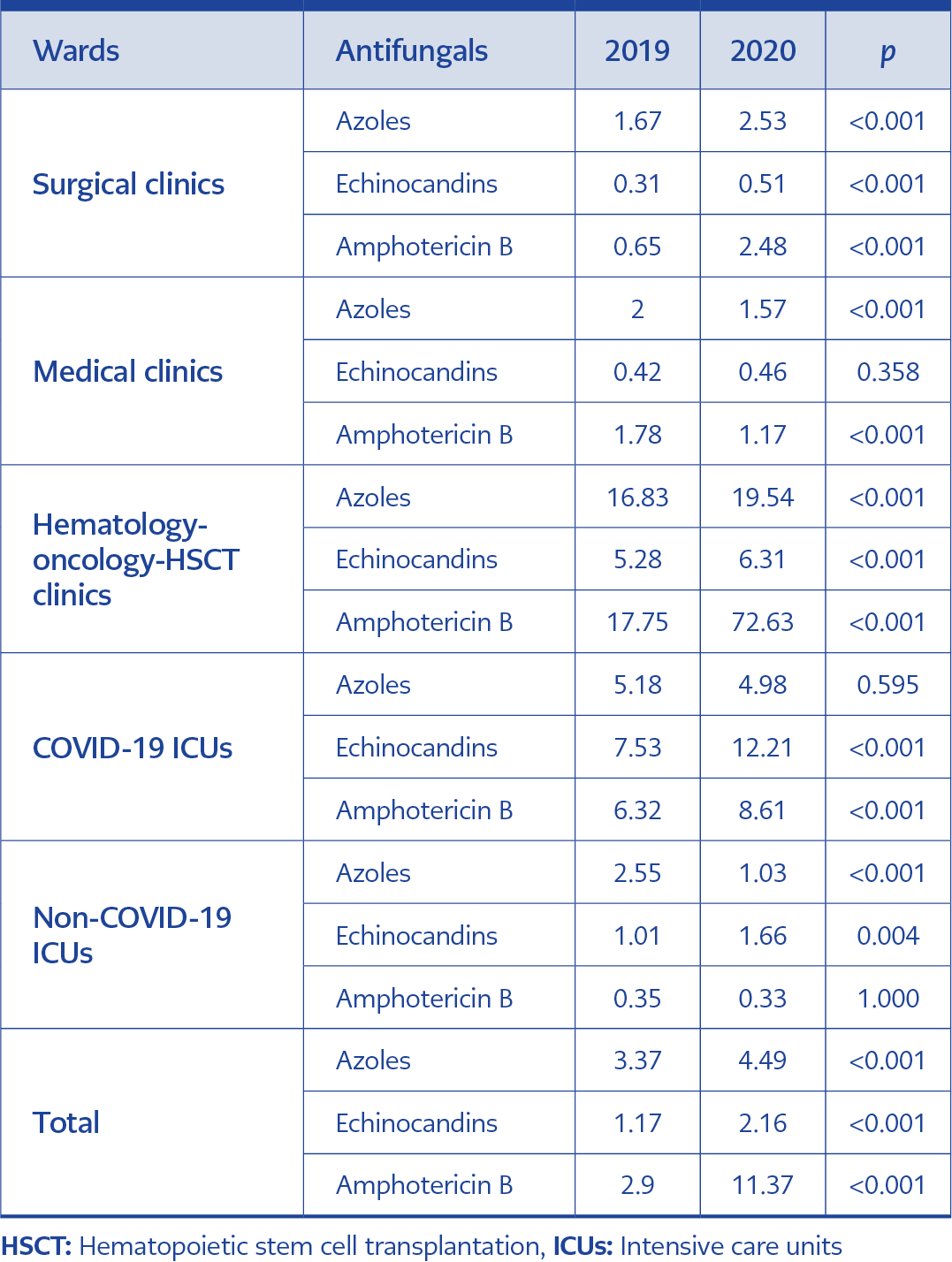
Table 3. The comparison of the consumption of different antifungal groups (azoles, echinocandins, and polyenes) by clinics (DDD/100 bed-days).
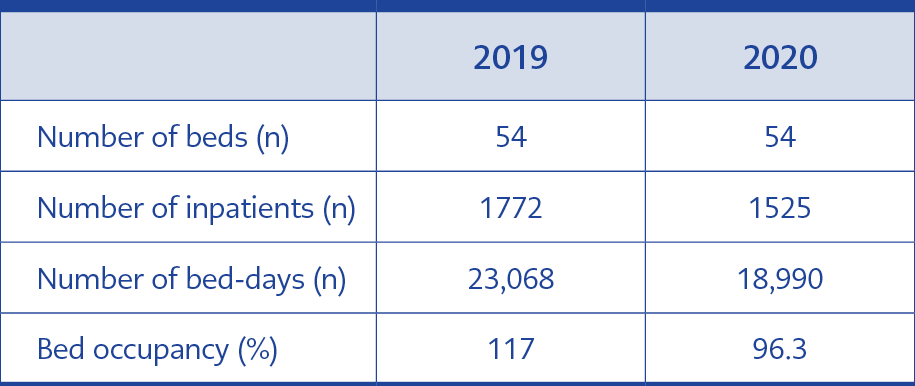
Table 4. Statistics of the number of beds, inpatients, hospitalization days, and the rate of bed occupancy in the hematology-oncology–HSCT clinics.
The antifungal consumption has statistically increased between 2019 and 2020 in the surgical clinics (2.62 vs. 5.52 DDD/100 bed-days, 95% CI=0.45-0.51, p<0.001), hematology-oncology-HSCT clinics (39.86 vs. 98.48 DDD/100 bed-days, 95% CI=0.39-0.42, p<0.001) and COVID-19 ICUs (19.03 vs. 25.80 DDD/100 bed-days, 95% CI=0.69-0.79, p<0.001). In the medical clinics (4.19 vs. 3.20 DDD/100 bed-days, 95% CI=1.22-1.41, p<0.001) and non-COVID-19 ICUs (3.92 vs. 3.01 DDD/100 bed-days, 95% CI=1.06-1.60, p=0.012) has statistically decreased. There was a statistically significant increase in antifungal consumption in all antifungal groups in the surgical clinics and hematology-oncology-HSCT clinics; liposomal amphotericin B consumption had a four-fold increase in both clinics. In COVID-19 ICUs, azole consumption has not changed, and echinocandin and polyene consumption has significantly increased. In the medical clinics, echinocandin consumption was the same between the two periods, azole and polyene consumption decreased. While echinocandin consumption has significantly increased in the non-COVID-19 ICUs, azole consumption has significantly decreased, and polyene consumption has not changed (Table 3).
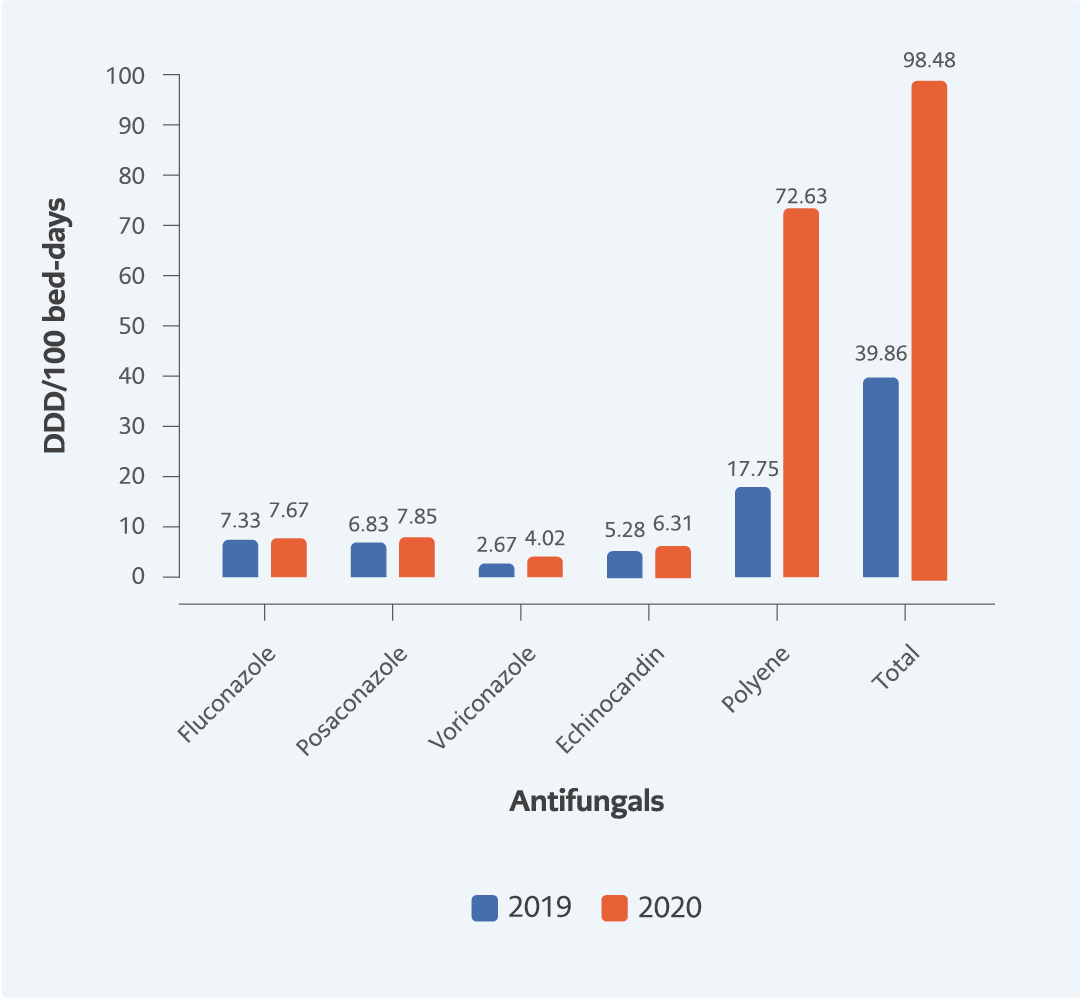
Figure 1. The distribution of antifungal consumption (DDD/100 bed-days) in the hematology-oncology-HSCT clinics.
There was no significant difference in the total number of beds, inpatients, and hospitalized days in the hematology-oncology-HSCT clinics (Table 4) in the pandemic period. The consumption of polyenes increased four-fold, significantly (95% CI=0.39-0.42, p<0.001). While the consumption of fluconazole did not change (95% CI=0.88-1.04, p=0.314), posaconazole (95% CI=0.80-0.95, p=0.002) and voriconazole (95% CI=0.58-0.76, p<0.001) have increased (Figure 1).
Discussion
In our study, the consumption of antifungals in the clinics during the pandemic increased two-fold. This increase was the highest in the hematology-oncology-HSCT clinics. Although antifungal use has been increasing with the increased numbers of immunosuppressive patients, it was reported that 30%-50% of antifungal use was inappropriate or unnecessary (7). Because the crucial laboratory tests for the diagnosis like aspergillus antigen, mycological, and cultures were unavailable, the radiologic examinations like the thorax computed tomography were limited, and performing bronchoscopies were interrupted, the empirical antifungal use was inevitable. Unnecessary use of antifungals can cause drug toxicities, drug interactions, and the selection of resistant fungal pathogens (8). Also, unnecessary use of antifungals increases the cost of hospital stay. Monitoring the consumption prevents collateral effects and reduces the cost. In this study, the increase in antifungal consumption in non-COVID-19 areas despite the decrease in the bed occupancy rate and the total number of hospitalized- days in the pandemic highlights the necessity of a novel approach for continuous communication through face-to-face meetings, telephone calls and text messages among clinicians, infectious diseases specialists, mycologists and radiologists. In a recent study from Türkiye, an AFS program managed by infectious disease specialists and clinical pharmacists increased the appropriate use of antifungals in the post-AFS period during the COVID-19 pandemic (9).
Although consumption increased in all antifungal groups during the pandemic, the highest increase was in the polyene (liposomal amphotericin B) group. This increase could be because liposomal amphotericin B has the broadest spectrum, and physicians in other specialties were unfamiliar with new antifungals. In our country, the use of antifungals has been under the control of infectious diseases specialists since 2003. However, it was reported that there were gaps in the knowledge of most physicians regarding the differentiation of fungal infection colonization, prophylaxis, empirical antifungal treatment indications, and antifungal selection (10). These gaps resulted in the use of broad-spectrum antifungal liposomal amphotericin B by false confidence. A study evaluating the candiduria approach in different specialties in our country reported that nearly half of the experts started treatment unnecessarily without excluding colonization and contamination (11). The increased consumption of anti-mold agents (liposomal amphotericin B and parenteral voriconazole) was not primarily related to the COVID-19-associated IFI, such as CAPA, the excessive consumption in Hematology-Oncology-HSCT clinics was more relevant.
In COVID-19 and non-COVID-19 ICUs, echinocandins were the most consumed antifungals. On the other hand, polyenes and anti-mold azoles were the most consumed antifungals in the hematology-oncology-HSCT clinics and azoles in the surgical clinics. This difference can be related to the differences in the most common type of fungus detected in different units; yeast species in the surgical clinics and ICUs and mold species in the hematology-oncology-HSCT clinics (12). In a study in which candidemia cases were evaluated in ICUs of six university hospitals in our region, including our center, it was reported that the most common cause was Candida albicans (13). The selection of the azoles in the surgical clinics and echinocandins in ICUs was expected, but the amount of consumption should be questioned. The excessive consumption of polyene in the hematology-oncology-HSCT clinics could result from impaired communication among disciplines and the lack of monitoring because of mandatory changes during the pandemic. Most of the physicians in our hospital preferred liposomal amphotericin B because it has low resistance rates and extended coverage for fungal species; they felt secure about the antifungal therapy. In the units with high antifungal consumption, sharing the data of their annually antifungal consumption and organizing regular education for appropriate antifungal usage can make a difference by updating awareness.
The use of echinocandins and polyenes in the COVID-19 ICUs was an empirical treatment for the patients’ underlying diseases and the COVID-19-related fungal infections. According to a study data in our center, the most common cause of fungal infections in COVID-19 intensive care patients was Candida spp. (14). It was also reported that the incidence of candidemia in COVID-19 patients requiring intensive care admission was 2.16 times higher than in non-COVID-19 patients (15). This information indicates that using empirical echinocandins in ICU patients, in line with the guidelines, was an expected finding.
There are several limitations of our study. First, it is a single-center, retrospective analysis. Second, we could not interpret the exact reasons for increased antifungal use because patient-based follow-up was unperformed due to a lack of data. Third, we could not determine the use of antifungals whether for treatment or prophylaxis, and the indications (such as Candidiasis, aspergillosis, cryptococcosis, etc.) for antifungal consumption because of the lack of the International Classification of Diseases, 10th Revision (ICD-10) coding for antifungal prophylaxis(16). We also had an indirect conclusion about the increased costs because we did not have a comparative cost analysis.
In conclusion, we observed a dramatic increase in antifungal consumption in the COVID-19 ICUs, surgical and hematology-oncology-HSCT clinics in the pandemic period. A novel approach for continuous communication among clinicians, infectious diseases specialists, internists, mycologists, and radiologists may decrease unnecessary and inappropriate antifungal use by monitoring consumption in the pandemic period.