Introduction
Clostridioides difficile is an anaerobic, Gram-positive, spore-forming bacteria found in the colon as part of the normal intestinal flora of a healthy individual. However, changes in the gut microbiota because of antibiotic use can lead to overgrowth of C. difficile and toxin production. As a result, C. difficile infection (CDI) develops, which is characterized by damage to the intestinal mucosa by C. difficile toxins. Antibiotic-associated diarrhea due to C. difficile is an important health problem that may be mild or may lead to hospitalization and even death. Antibiotic use is the most common risk factor, additional risk factors for disease development include advanced age, history of hospitalization and comorbid conditions (1-5). The primary recommended method for the diagnosis of the disease has been reported as a nucleic acid amplification test (6).
Recurrent C. difficile infection (rCDI) is defined as the resumption of symptoms within eight weeks after the onset of the first episode in patients whose complaints and findings have improved after appropriate treatment (7). Once recurrence develops, repeated attacks are likely to occur. Therefore, it is important to identify risk factors for patients who will develop recurrence. Advanced age, use of proton pump inhibitors (PPI), infection with hypervirulent strains, severe underlying disease, previous episode severity, prolonged hospitalization and antibiotic use for non-C. difficile infection after diagnosis are previously reported risk factors for rCDI (8).
In this study, we aimed to investigate the characteristics of C. difficile infections followed up in our hospital and to investigate the factors associated with recurrence.
Materials and Methods
Study Design and Population
The study was retrospectively conducted at Giresun Training and Research Hospital between September 2021 and December 2023. Adult patients (18 years and older) with clinical signs of acute gastroenteritis and who were tested with gastrointestinal polymerase chain reaction (GI PCR) panel test from stool material and identified as C. difficile pathogen were included in the study. Patients with signs of acute gastroenteritis but no GI PCR panel test performed or non-C. difficile pathogens detected in the panel test were excluded.
Patients’ data were obtained from hospital medical electronic file records. Age, gender, hospitalization status (outpatient, ward admission or intensive care unit admission), comorbidities, Charlson comorbidity index, PPI use, history of hospitalization in the last three months, history of gastrointestinal procedures in the last month, statin use, antibiotic use in the last two months, leukocyte count, serum creatinine, serum albumin, infection severity, treatment administered for CDI, recurrence status, 28-day mortality, all-cause mortality during hospitalization, need for intensive care unit stay were recorded. Demographic and clinical data and outcomes of CDI patients were evaluated. Variables in patients with and without recurrence were compared, and risk factors for recurrence were investigated.
Definitions
Severe infection was defined as a patient with a leukocyte count >15,000 cells/mL, serum creatinine >1.5 mg/dL or serum albumin <3 g/dL.
rCDI was defined as the recurrence of symptoms within eight weeks after the onset of the first episode in patients whose symptoms improved with appropriate antimicrobial treatment and the detection of C. difficile again in the GI PCR panel.
Hospital-acquired infection was defined as diarrhea developing in a patient who had no symptoms and signs at admission and who had been hospitalized for at least 48 hours and C. difficile was detected in the GI PCR panel.
The presence of immunosuppression was defined as receiving chemotherapy treatment for cancer, use of immunosuppressive biological drugs for systemic autoimmune disease, or use of corticosteroids equivalent to prednisone at a minimum dose of 20 mg/day for more than 14 days.
Microbiology
Stool samples of patients with diarrhea sent to the laboratory in transport medium were analyzed by multiplex real-time polymerase chain reaction (Rt-PCR) method with QIAstat-Dx Analyzer 1.0 (Qiagen N.V., Germany) instrument and QIAstat-Dx Gastrointestinal Panel 2 (Qiagen N.V., Germany). The collected fresh stool sample was resuspended in a Cary-Blair transport medium (Copan, Italy). Two hundred microliters of the liquid sample were manually loaded into the QIAstat-Dx Gastrointestinal Panel 2. Extraction, amplification and detection of nucleic acids in the sample were performed automatically by QIAstat-Dx Analyzer 1.0. The liquid sample is homogenized, and cells are lysed in the lysis chamber of the QIAstat-Dx Gastrointestinal Panel 2, which contains a high-speed rotating rotor and silica beads for efficient cell lysis. Nucleic acids are purified from the lysed sample by binding to a silica membrane in the purification chamber of the QIAstat-Dx Gastrointestinal Panel 2 in the presence of chaotropic salts and alcohol. Purified nucleic acids are eluted from the membrane in the purification compartment and mixed with lyophilized PCR chemistry in the dried chemistry compartment of the QIAstat-Dx Gastrointestinal Panel 2. The mixture of sample and PCR reagents is dispensed into the QIAstat-Dx Gastrointestinal Panel 2 PCR chambers containing air-dried assay-specific primers and probes. The QIAstat-Dx Analyzer 1.0 creates the optimal temperature profiles to carry out effective multiplex Rt-PCR and performs Rt-fluorescence measurements to generate amplification curves. The QIAstat-Dx Analyzer 1.0 software interprets the resulting data and process controls and delivers a test report. Patients with C. difficile toxin A and B genes detected by this method were evaluated as CDI.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 26.0 (IBM Corp., Armonk, NY, USA). Mean, standard deviation, percentages and median (minimum-maximum) were used for descriptive statistics. Compliance of quantitative data with normal distribution was evaluated using the Kolmogorov-Smirnov test. Mann-Whitney U test was used to compare quantitative data. The chi-square test or Fisher’s exact test was used to compare the percentages between independent groups. To investigate independent risk factors for recurrence, multivariate logistic regression analysis was performed with variables with p<0.100 in univariate analysis. The statistical significance was set as p<0.05.
Results
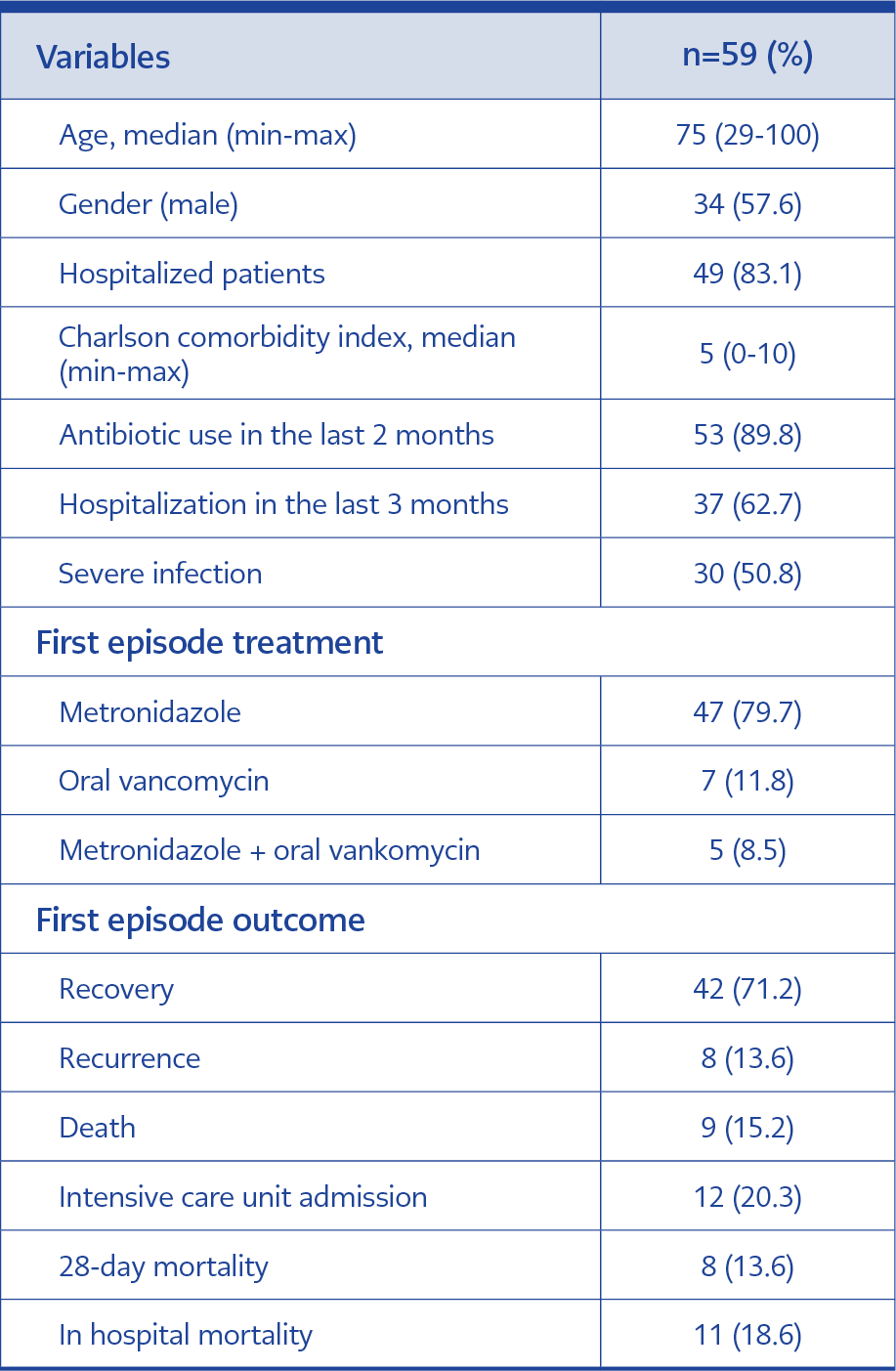
Table 1. Demographic and clinical characteristics of Clostridioides difficile patients.
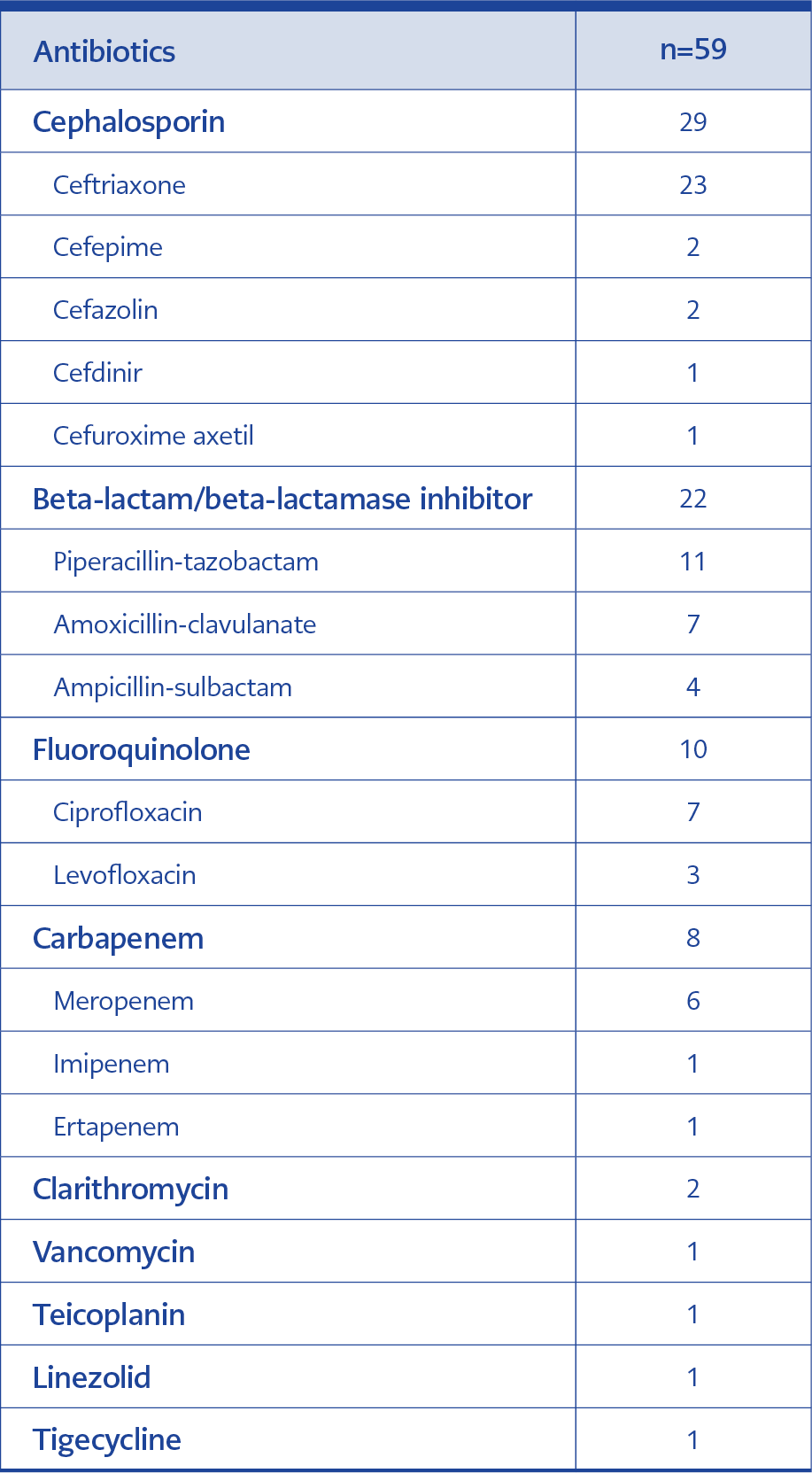
Table 2. Antibiotics used by patients with Clostridioides difficile before the first episode.
A total of 669 GI PCR panel tests were performed during the study period, and 384 were positive for a causative agent. In samples where only one agent was detected, the distribution was as follows: Enteropathogenic Escherichia coli (EPEC) in 115 patients, C. difficile in 59 patients, norovirus GI/GII in 42 patients, enteroaggregative E. coli in 37 patients, Shiga-like toxin-producing E. coli (STEC) in 34 patients, Campylobacter spp. in 29 patients, enterotoxigenic E.coli in 22 patients, rotavirus A in 12 patients, Salmonella spp. in ten patients, sapovirus (GI, GII, GIV, GV) in seven patients, Giardia lamblia in four patients, Cryptosporidium spp. in three patients, enteroinvasive E. coli/Shigella in three patients, astrovirus in three patients, adenovirus F40/F41 in two patients, STEC serotype O157:H7 in two patients. Among these patients, 59 CDIs were diagnosed. The median age of the patients was 75 years, 57.6% were male. The number of patients diagnosed during hospitalization was 49 (83.1%). Metronidazole was the most commonly used drug for the treatment of CDI. Demographic and clinical data of the patients and the outcomes are shown in Table 1. Fifty-three (89.8%) patients had a history of antibiotic use before CDI. The most frequently used antibiotics were ceftriaxone, piperacillin-tazobactam, amoxicillin-clavulanate and ciprofloxacin, respectively. Details of antibiotics used before CDI are shown in Table 2.
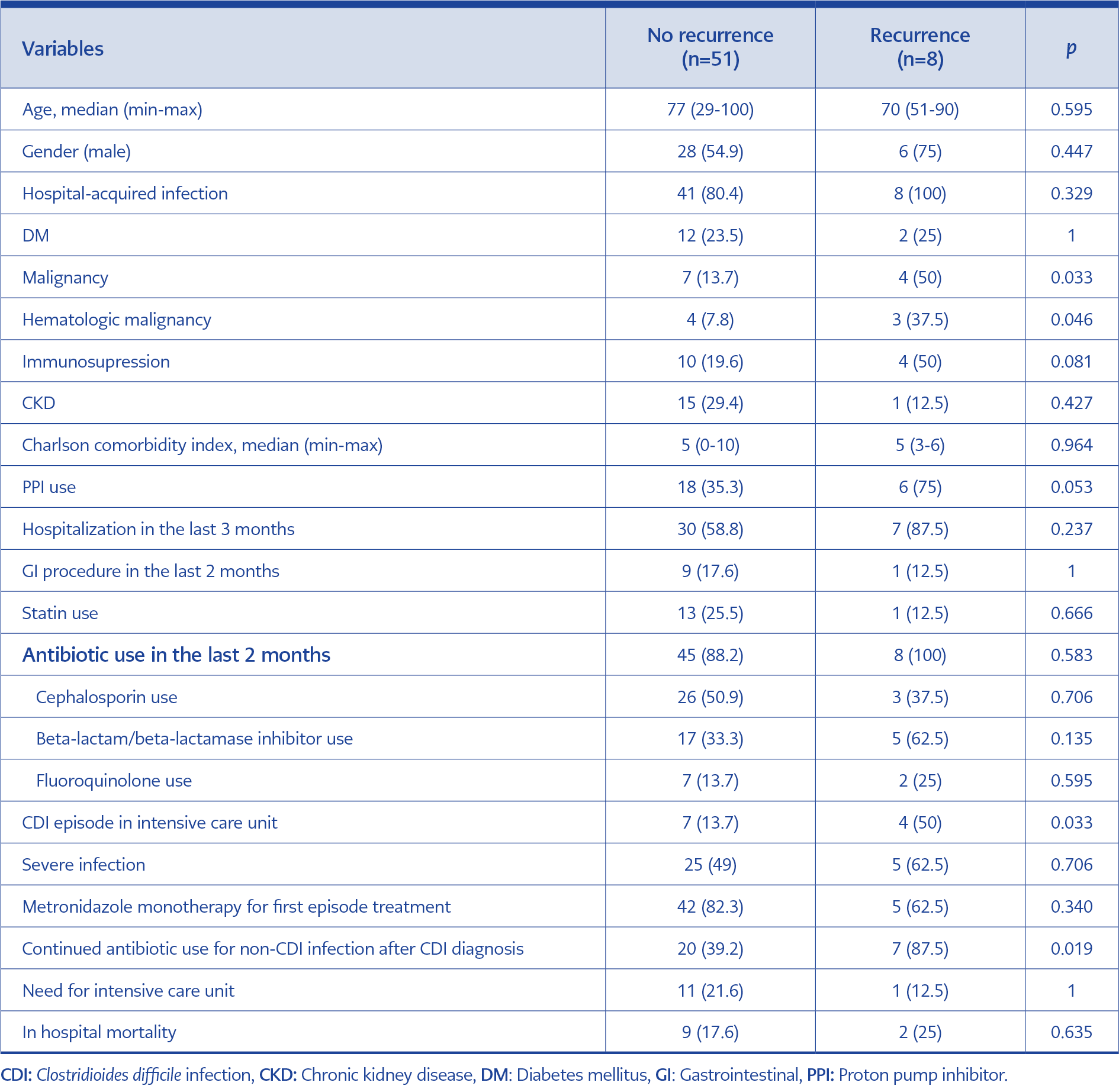
Table 3. Comparison of Clostridioides difficile infections with and without recurrence.
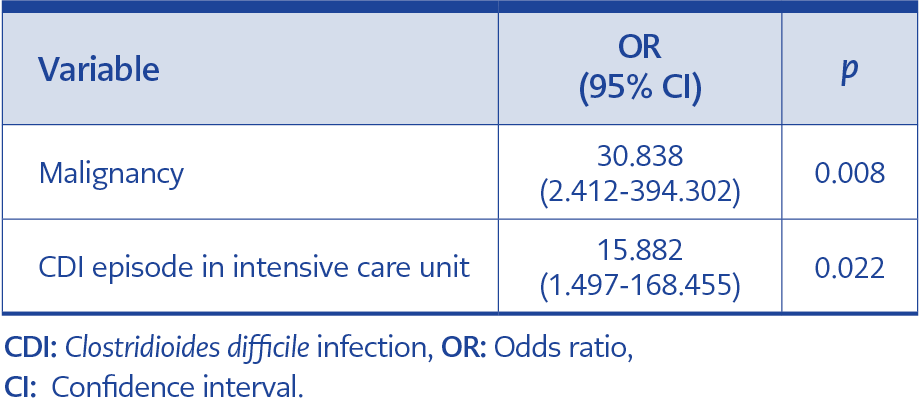
Table 4. Logistic regression analysis for risk factors associated with recurrence.
A total of eight patients developed rCDI. The development of recurrence was observed in 21.4±11.6 days after the onset of the first episode. In the rCDI group, the presence of malignancy and hematologic malignancy, the development of CDI episodes in the intensive care unit, and the continuation of antibiotic treatment for non-C. difficile agent after diagnosis of CDI were statistically more frequent (p<0.05). The presence of immunosuppression and use of PPI before the infection were more common in rCDI group, but statistical significance was not found. The comparison of patients with and without recurrence is shown in Table 3. A model was created to identify independent risk factors for rCDI, including malignancy, hematologic malignancy, immunosuppression, PPI use, CDI episodes in the intensive care unit and continued antibiotic use for non-CDI infection after CDI diagnosis. Malignancy and CDI episode in intensive care unit were determined as independent risk factors for recurrence (Table 4).
While mortality was not observed in any outpatient patient, mortality developed during hospitalization in 11 (18.6%) patients. Of these, nine were during the first episode, and two were during recurrence. Among the patients who developed mortality, the rate of infection in the intensive care unit was 54.4%, the rate of antibiotic treatment continuation for non-C. difficile cause after diagnosis was 90.9%, and the rate of severe infection was 100%. These three variables were statistically significantly more frequent in the mortality group compared to the non-mortality group (p=0.003, p=0.001, p<0.001, respectively). The median age was 84 years in the mortality group and 75 years in the survivors, but there was no statistically significant difference.
Discussion
C. difficile is an important cause of antibiotic-associated diarrhea. The disease may have a mortal course, especially in patients with comorbid conditions. In many studies conducted worldwide, it has been reported to be one of the most common cause of gastroenteritis (9, 10). In a recent study of 175 cases of acute gastroenteritis reported from our country, C. difficile was found to be the second most common pathogen (11).
The disease is important because of its frequency and more severe course compared to most other gastroenteritis agents. In addition, C. difficile is an important cause of nosocomial diarrhea (12). In our study, clinical characteristics, outcomes and recurrence-associated factors of C. difficile patients diagnosed in our hospital were analyzed. Due to its high sensitivity, GI PCR may show false positive results in cases such as asymptomatic carriage and colonization. There are reports that cases with a positive PCR test but no toxin detected by immunoassay may receive an unnecessary diagnosis of C. difficile (13). To avoid unnecessary diagnosis, PCR test is recommended in patients with three or more loose stools in 24 hours (6, 14). In our study, in order to exclude these cases, liquid stool material from patients with signs of acute gastroenteritis (three or more watery stools in 24 hours) was evaluated as previously recommended.
When examining the characteristics of the study population, the advanced age, the high incidence of infection occurring during hospitalization, the high median value of the Charlson comorbidity index, and a history of antibiotic use in 53 patients within the last two months stand out as prominent features. These variables have previously been reported as risk factors for CDI (15). All antibiotics potentially pose a risk for CDI, but cephalosporins, fluoroquinolones, clindamycin and beta-lactam/beta-lactamase inhibitors, in particular, greatly increase the risk (16). Cephalosporins, beta-lactam/beta-lactamase inhibitors and fluoroquinolones were the most frequently used antibiotics in our study population in the last two months before diagnosis. The main reason for this is that these antibiotic groups are broad-spectrum and highly effective on gastrointestinal flora.
In our center, metronidazole was the most commonly used antibiotic for the treatment of C. difficile. The use of oral vancomycin in monotherapy or combination therapy was observed in 12 patients. In the guidelines published in the United States of America (USA) for the treatment of C. difficile, fidaxomycin was recommended as the first choice for the treatment of the first episode. Alternatively, oral vancomycin and metronidazole (if not severe infection) were recommended (17). In our country, fidaxomycin is not reimbursed, and its use is limited due to its high cost. For this reason, it was observed that treatments other than fidaxomycin were commonly used in the study population.
In a study conducted in our country involving pediatric patients between the ages of 2-18 years, mortality in the course of hospital-acquired CDI was reported to be 5.3% (18). To our knowledge, there is no report in the literature regarding mortality in adult patients with CDI in our country. C. difficile has been found to be the leading cause of gastroenteritis-related deaths in studies conducted in the USA (19, 20). In one study, one-year all-cause mortality after CDI was reported to be 40.9% (21). Among the patients in our study, mortality did not develop in outpatients. All-cause mortality during hospitalization was found to be 18.6%. It was observed that all patients with mortality were patients with severe infection. The continuation of antibiotic treatment for non-C. difficile infection after CDI diagnosis and the development of the disease in the intensive care unit was found to be associated with mortality.
rCDI poses a significant challenge in the treatment and follow-up of patients with CDI. In our study, the recurrence rate was 13.6%. Studies conducted in different centers have reported recurrence rates between 13.5% and 20.9% for community-acquired and hospital-acquired cases (19, 22). In studies investigating factors related to recurrence, severe CDI, presence of inflammatory bowel disease, exposure to cephalosporins, advanced age, gastric acid-suppressing therapies, presence of underlying severe comorbid disease, presence of previous CDI, serum creatinine value ≥1.2 mg/dL, and use of additional antibiotics other than CDI treatment have been found as risk factors in different studies (8, 22-25).
In our study, the presence of malignancy, hematologic malignancy, development of CDI episode in intensive care unit, and continued use of antibiotics for infections other than CDI after diagnosis were found to be significantly higher in the rCDI group. In logistic regression analysis, presence of malignancy and CDI infection developed in intensive care unit were determined as independent risk factors for recurrence. It was thought that the effects of malignant processes on the immune system and the additional use of heavy immunosuppressive treatments such as chemotherapy may complicate the treatment of the disease in these patients and lead to recurrence. Due to factors such as immunosuppression, impaired enteral nutrition, polypharmacy (gastric acid suppressor drugs such as PPIs), hemodynamic instability and changes in gastrointestinal flora, which are frequently seen in critically ill patients in the intensive care unit, may contribute to the recurrent course of CDI episode in the intensive care unit. Antibiotic use is an important risk factor for C. difficile both in the development of disease and in the development of recurrence. It is not surprising that the use of non-CDI antibiotic treatment for a different infection while receiving treatment for a CDI episode is common among the group that experiences recurrence due to its negative effect on intestinal flora. Advanced age, which has been found to be associated with recurrence in many previous studies, was not found to be associated with this condition in our study. Since the median age of the patients in our study was 75 years and only 14 patients were under 65 years of age, in other words, it was already a very elderly population, the effect of advanced age on recurrence could not be demonstrated. In addition, although immunosuppression and PPI use were more frequent in the group with recurrence in our study, statistical significance was not found.
The limitations of our study include its retrospective and single-center design, limited sample size, lack of hypervirulent strain evaluation and lack of evaluation of antibody-related immune response to C. difficile toxins.
In conclusion, to the best of our knowledge, our study is the first study on recurrence in C. difficile patients reported from Türkiye. The frequency and high mortality rate of the disease is remarkable. Evaluation of patients who may develop recurrence in terms of risk factors and close follow-up will help improve the outcomes of the disease. Prospective and more comprehensive studies to be conducted in our country will contribute to the management of the disease.