Introduction
With the prolongation of life expectancy and the developments in orthopedic surgery, noteworthy progress has been made in prosthetic joint surgery in recent years. Joint replacement provides pain relief, improves quality of life, and gives independence to individuals. Along with the advances in prosthetic surgery, prosthetic joint infection (PJI) is still the most feared complication of the procedure. PJI leads to prolonged hospitalization, repetitive surgery, prolonged use of antibiotics, even removal of the prosthesis, loss of joint function, and death in some cases. Around 1 million arthroplasties are performed in the United States, and increasing numbers are recorded all over the world every year (1, 2). The need for arthroplasty is expected to increase by 400% from the early 2000s to 2030, possibly further increasing the prevalence of PJI (3). The rate of PJI varies from 0.5% to 2% for hip and knee replacements (4). The 1-year cumulative mortality rate in patients with PJI is 5.5-8%; the 10-year mortality rate is reported to be 10-38% (5-7). Also, the economic burden of the disease is high, approximately 1.5-4 times higher than the cost of primary prosthesis surgery (8, 9).
Anamnesis, clinical signs and symptoms, infection markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), imaging, microbiological and histopathological examination of joint fluid, and periprosthetic tissue samples are used together for the diagnosis of PJI. Antibiotics and surgery are used in combination for treatment (10, 11). Making individual plans with appropriate medical and surgical approaches is important for improving the patient’s quality of life. All the parameters involved in the follow-up, therapy, and effectiveness of once-daily antibiotics should be investigated in detail for treatment achievement.
This study aimed to find the most practical approach to PJI and evaluate the effectiveness and usability of teicoplanin in treating PJI. Thus, we evaluated the parameters used in the follow-up, surgical methods, and antibiotic treatments and the factors affecting the treatment response, especially the effectiveness and usability of teicoplanin, a once-daily and well-tolerated antibiotic.
Materials and Methods
Patient selection and data collection
This study included patients followed up in a tertiary education and research hospital between January 2010 and December 2017, with the diagnosis of Gram-positive or culture-negative PJI, who were over 18 years of age and followed up for more than three months after completion of treatment procedures. Gram-negative PJIs were excluded from the study because the study aimed to evaluate the effectiveness of teicoplanin. Also, patients who died due to reasons other than PJI within the treatment period were excluded. PJIs that occurred because of different microorganisms or developed at least two years after the first infection were considered different infections. Patients’ data was recorded retrospectively from the hospital information system. The Yıldırım Beyazıt University Medical Faculty Clinical Research Ethics Committee approved the study on April 13, 2016, with the decision number 113.
Definitions
The Infectious Diseases Society of America (IDSA) 2013 diagnostic criteria were used to diagnose PJI. “Zimmerli/Trampuz Classification,” which is the classification system also accepted by IDSA, was used for infection classification (12). Treatment response was defined as the eradication of infection (healing of infected wound or fistula, no discharge, no pain, no reinfection with the same microorganism), no need for additional surgical intervention, and no PJI-related mortality (sepsis or necrotizing fasciitis); in the presence of any of these, patients were considered to be non-responders (10).
Microbiological study
Differential cell count, gram staining, and culture were studied in synovial fluid, and tissue samples were taken pre- or intraoperatively. The samples were incubated for at least five days, and if growth was detected, the microorganisms were identified by traditional methods.
Treatment
The treatment plan was done according to the time of the infection, the joint condition, the patient’s characteristics, the causative microorganism, the surgeon’s experience, and the patient’s request, as suggested (13). A combination of surgery and antimicrobial therapy was the main therapeutical approach. After diagnosing PJI, the orthopedist decided on the surgical procedure, and the infectious diseases specialists planned the antibiotic therapy.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 21.0 (IBM Corp., Armonk, NY, USA). Demographic data was evaluated according to the number of patients, and other findings were evaluated according to the number of PJIs. Demographic data, PJI-related variables, and treatment-related data of the study were expressed as numbers and percentages. The normal distribution of variables was examined using Kolmogorov-Smirnov or Shapiro-Wilk tests. Descriptive analyses were given using mean ± standard deviation for normally distributed data and median (interquartile range, IQR) for not normally distributed data. The difference between the groups was compared using the Chi-square or Fisher tests. Numerical data were compared with the t-test to evaluate if the data was normally distributed and with Mann-Whitney U if not. In multivariate analysis, independent predictors of treatment response were examined with logistic regression analysis using possible factors identified in previous analyses. The Hosmer-Lemeshow test was used to determine the model fit. The statistical significance was set as p<0.05.
Results
Of the 244 patients followed during seven years, 169 PJI episodes of 151 patients who met the study criteria were included. Of the patients, 98 (64.9%) were male, and the mean age was 67±10 years. The majority of infections were knee PJIs (115; 68%), followed by hip (50; 29.6%), shoulder (3; 1.8%), and elbow (1; 0.6%) PJIs. Among them, 119 (70.4%) were primary prostheses, 21 (12.4%) were revision prostheses because of infection, and 16 (9.4%) were revision prostheses due to mechanical reasons. Early infection was detected in 33 (19.5%), delayed infection in 48 (28.4%), and late infection in 88 (52.1%) patients’ prosthetic joints.
Intraoperative or preoperative cultures were not taken in four patients. The pathogen could not be identified in 26% of the infections, and 11% of the PJIs were polymicrobial. The most frequently identified Gram-positive microorganism was coagulase-negative staphylococci, 37% methicillin-resistant and 26% methicillin-sensitive strains. Staphylococcus aureus accounted for 17% of the pathogens (12% methicillin-sensitive and 5% methicillin-resistant), followed by Enterococcus spp. (15%) and Streptococcus spp. (5%).
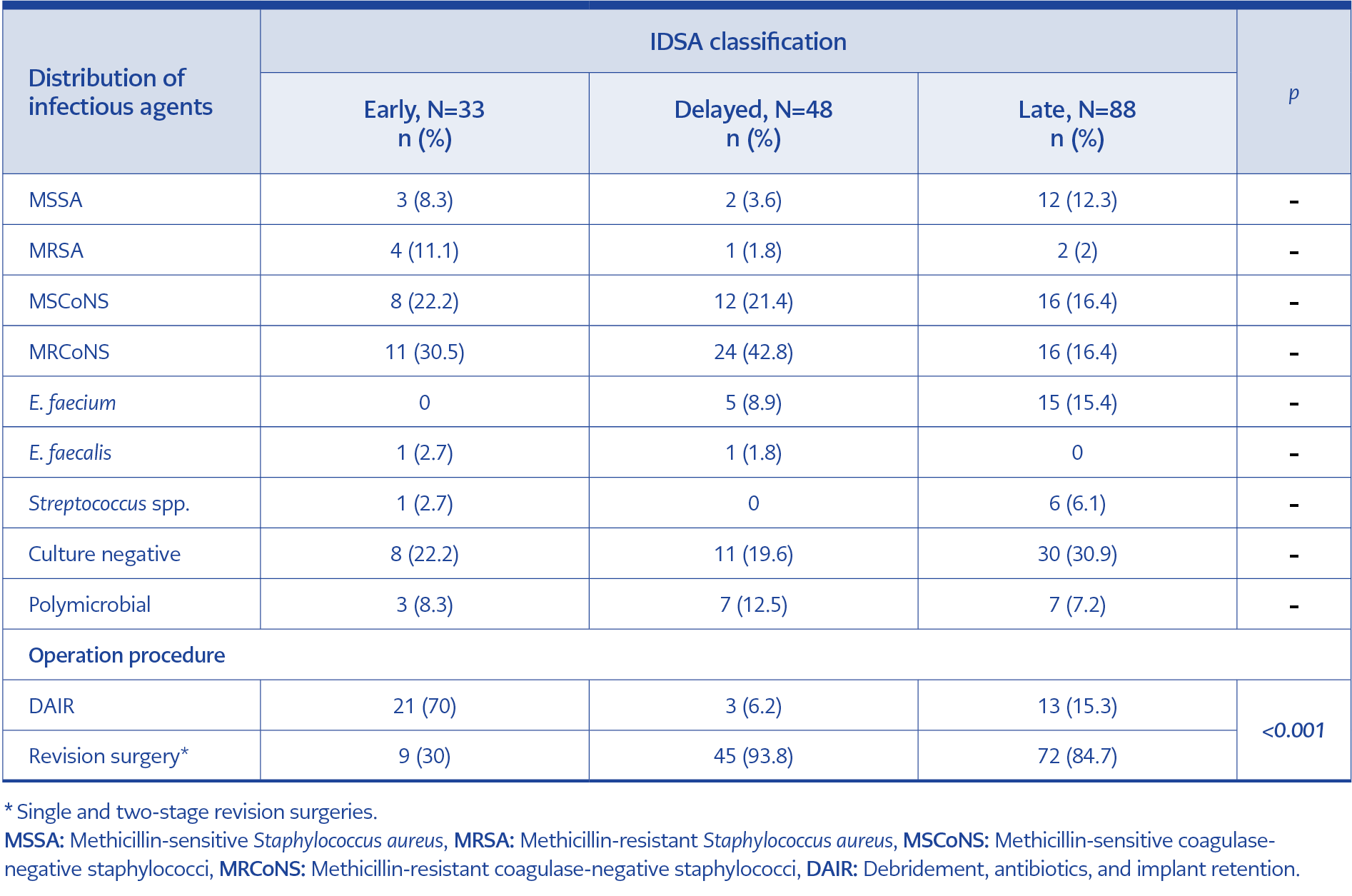
Table 1. Distribution of infectious agents and surgical procedures according to IDSA classification.
Debridement, antibiotics, and implant retention (DAIR) procedure was applied to 37 (21.8%) of the PJIs followed, one-stage revision surgery to 5 (2.9%), two-stage revision surgery to 121 (71.5%), and resection arthroplasty to 3 (1.7%). Only antibiotic treatment was applied to 3 (1.7%) patients followed. While the DAIR procedure was applied to mostly patients with early infection, revision surgery (single or two-stage) was applied to mostly those with delayed and late infection (p<0.001, Table 1). Two-stage revision surgery was applied to 75% (n=12) of the patients we followed and who failed to cure after DAIR (n=16), and treatment response was obtained in 83% (n=10) of them. Likewise, resection arthroplasty and joint arthrodesis were applied to two patients whose treatment was not successful after two-stage revision.
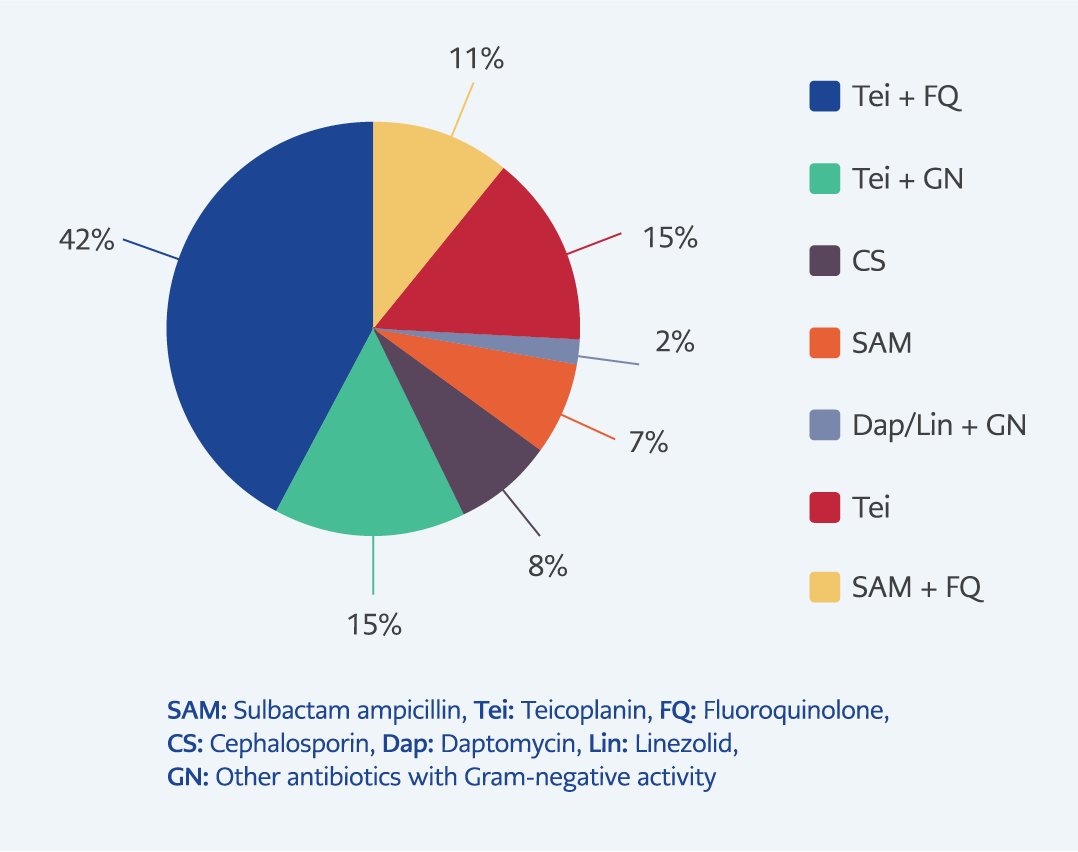
Figure 1. Parenteral antibiotic treatments.
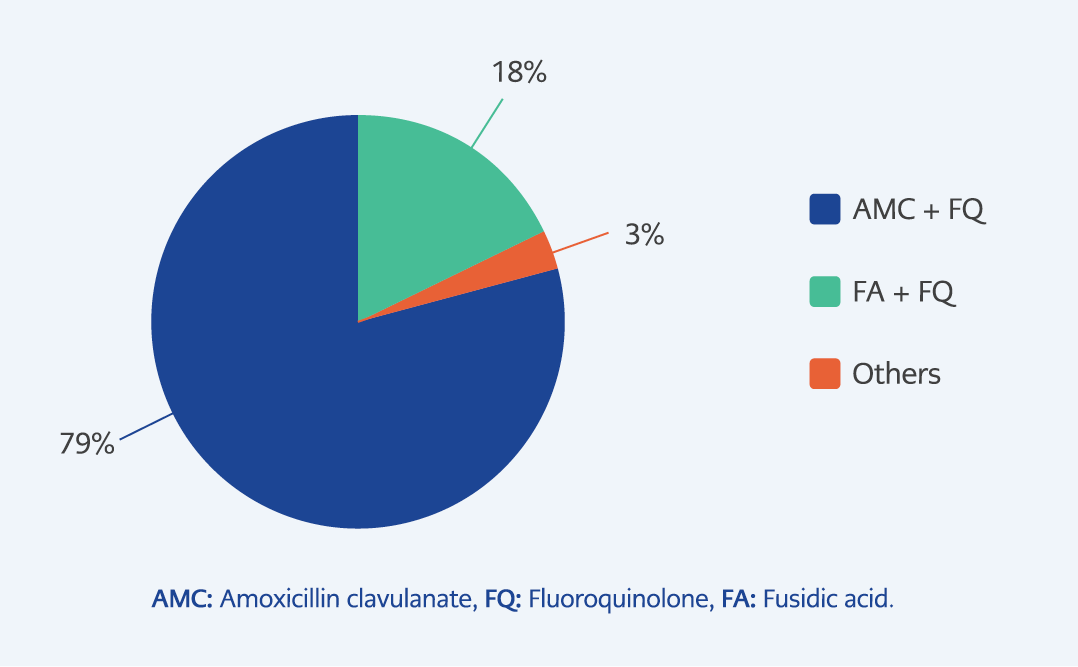
Figure 2. Per oral antibiotic treatments.
While 162 (96.4%) patients used parenteral and per-oral antibiotic combination, 6 (3.6%) had only oral antibiotic therapy. The most administered parenteral antibiotic is the combination of teicoplanin and fluoroquinolone, and per-oral therapy is amoxicillin clavulanate alone or in combination with fluoroquinolone (Figure 1, Figure 2). Teicoplanin given to 131 (77.5%) patients. The mean initial parenteral antibiotic duration of patients who underwent the DAIR procedure was 7 ± 6 weeks, and the total treatment duration was 19 ± 10 weeks. For patients who underwent two-stage revision surgery, these periods were 6±5 weeks and 9 ± 5 weeks, respectively.
Treatment response was evaluated in 168 of 169 PJIs included in the study, but one patient could not be included because of missing data. After the completion of surgical and medical treatment, 139 (82.7%) of PJI episodes were defined as treatment responders.
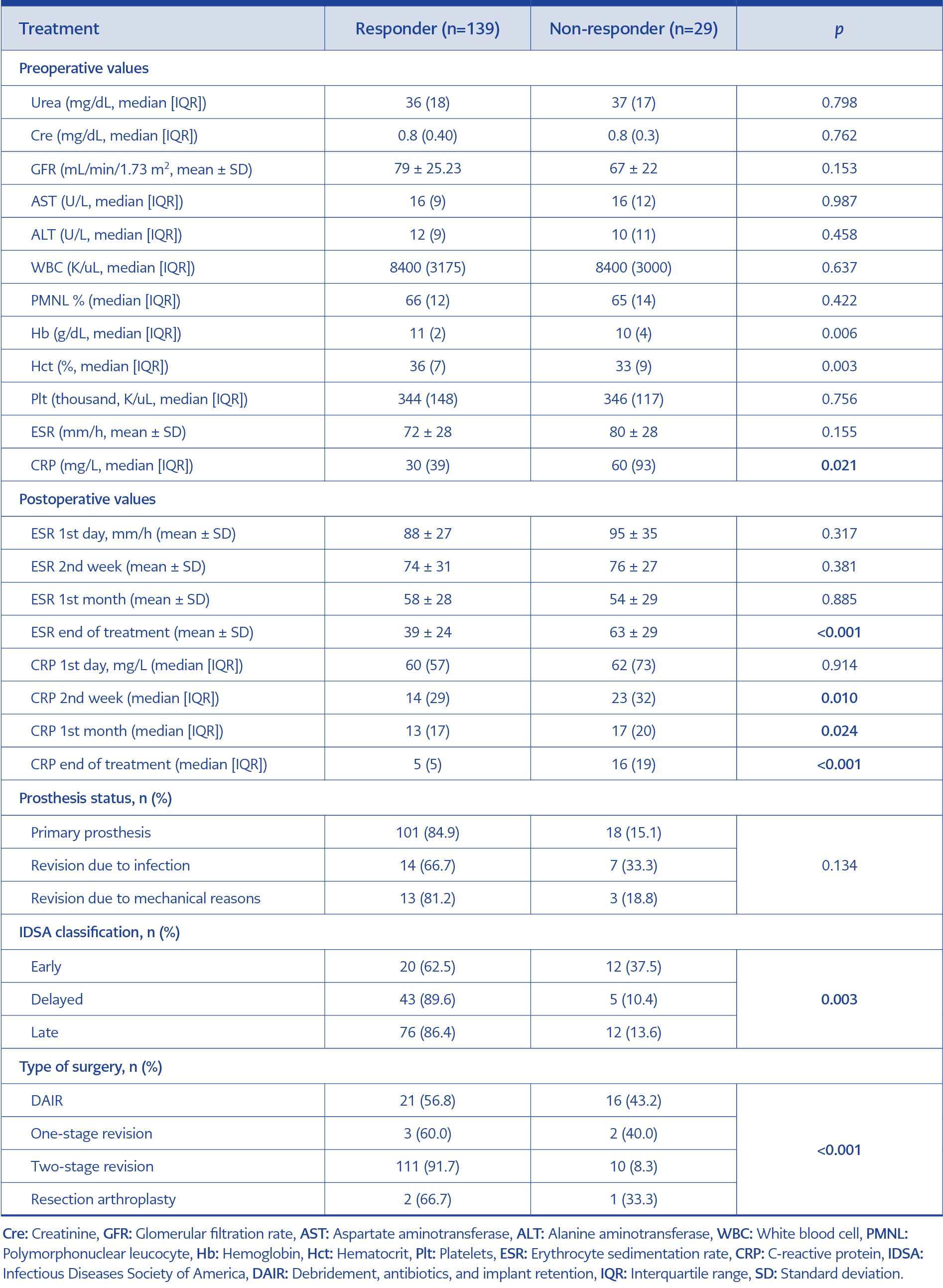
Table 2. Factors affecting treatment response.
Factors affecting treatment response in the pre-and postoperative periods were examined (Table 2). The treatment failure rate was higher in early infections than in delayed and late infections (p=0.003). In the treatment responder group, preoperative hemoglobin (Hb) and hematocrit (Hct) values were higher, and CRP levels were lower than the non-responder in the preoperative period (p=0.006, p=0.003, p=0.021, respectively). White blood cell, polymorphonuclear leucocyte (PMNL) %, renal function tests, and liver function tests had no significant effect on treatment response. The treatment success rate was higher in patients with lower ESR and CRP levels; besides, the relationship between the CRP value and the treatment response emerged in an earlier period than ESR (second week for CRP and end of treatment for ESR, Table 2). The treatment response was obtained in most of the patients who underwent two-stage revision surgery; however, the lowest treatment response was in the DAIR group. The difference was statistically significant (p<0.001) (Table 2).
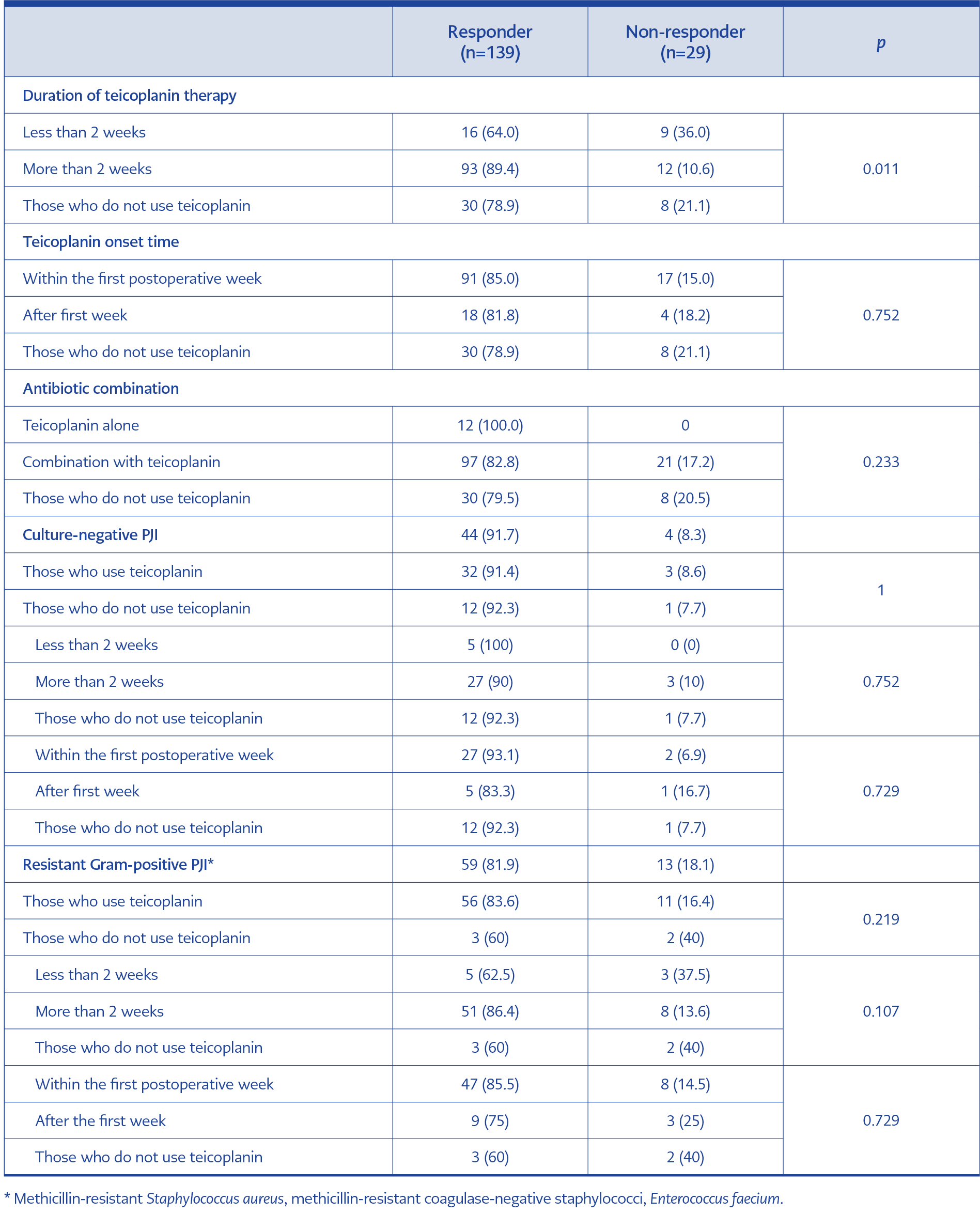
Table 3. Effect of teicoplanin on treatment response.
In addition, the use of teicoplanin in the treatment of PJI was separately evaluated. While 78.9% of patients who did not use teicoplanin responded positively to the treatment, this rate was 89.4% for those who used it for two weeks or more. Combining teicoplanin with another antibiotic did not contribute to the treatment response (p=0.243) (Table 3). In the subgroup analysis of culture-negative and resistant Gram-positive PJIs, teicoplanin did not significantly affect treatment response (Table 3).
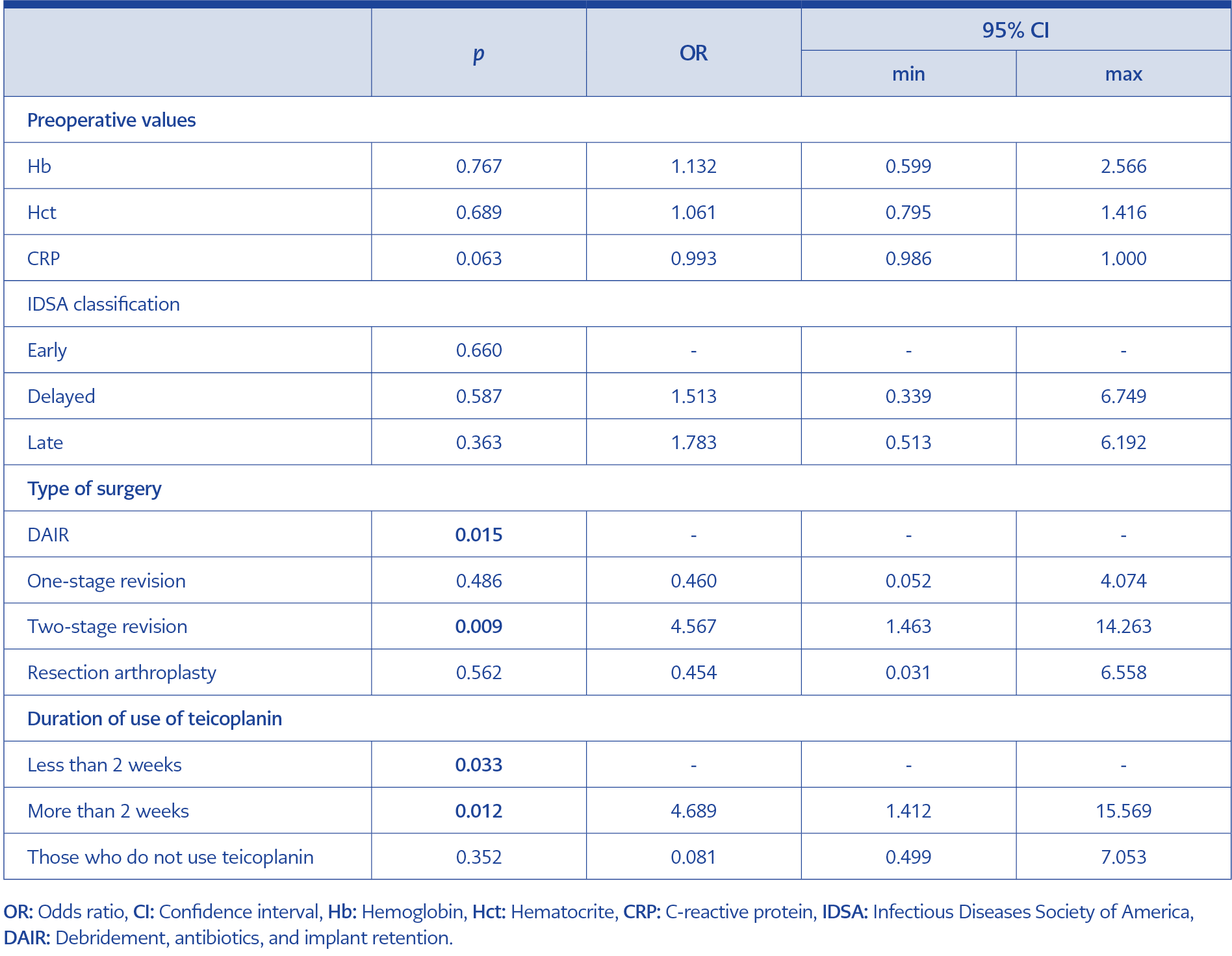
Table 4. Factors affecting treatment response; multivariate analysis.
Parameters affecting treatment response in univariate analysis were evaluated by logistic regression analysis. Among surgical methods, the two-stage revision surgery success rate was higher compared to other methods (odds ratio [OR]=0.009; 95% confidence interval [CI]=1.463-14.263). Also, using teicoplanin for two weeks or more seemed to increase the treatment response (OR=4.689; 95% CI=1.412-15.569) (Table 4).
Discussion
The treatment was successful in 82.7% of the 169 patients included in our study. Although it was not significant in multivariate analysis, low preoperative Hb and Hct and high CRP may be important in indicating treatment failure. The effect of CRP in follow-up occurs earlier than ESR. CRP monitoring, especially beginning from the second postoperative week, may be effective in predicting treatment response. The success rate of two-stage surgeries is higher than other surgical methods. Teicoplanin, which can be used as an outpatient parenteral antibiotic treatment (OPAT) once a day and has fewer side effects than other glycopeptides, is a suitable and effective choice for treating PJI.
With the ageing population, joint dysfunctions became more common, and the importance of arthroplasty increased. PJI is a challenging process for both the patient and the attending physician. The experiences of PJI centers are more important than ever in finding the best approach for each individual, such as laboratory tests to be used, surgeries, and antibiotic treatments to be applied.
Determining the factors affecting treatment response allows both appropriate interventions in the preoperative period and the selection of the right treatment in the postoperative period. Identifying risky patients and treating and following up with this group more carefully is important. The rate of PJI development is 1.1-2.5% in primary knee prostheses and 0.7-1.7% in hip prostheses. In revision prostheses, regardless of the reason for revision, the rate of PJI development is higher than in primary prostheses. Also, previous PJI is considered among nonmodifiable preoperative risk factors (14).
Anemia can cause tissue hypoxia and even systemic inflammation. In two different studies, including PJI, hemoglobin levels below 10 g/dL and hematocrit levels below 32.1 in the preoperative period were associated with treatment failure (15, 16). In our study, Hb and Hct were lower in the treatment non-responder group than in responders in the preoperative period, but this difference was not significant in multivariate analysis. Treating anemia before surgery in patients followed up with a diagnosis of PJI may increase the treatment response.
ESR and CRP are the most valuable laboratory parameters in diagnosing and following PJI (11, 13, 17). In a study evaluating the factors associated with treatment failure following DAIR, an ESR value exceeding 60 mm/hr was identified as a predictor of treatment failure (18). Also, in a study evaluating the treatment response in PJIs, a CRP level above 22 mg/L at the time of admission was associated with failure. In contrast, in another, a CRP value above 100 mg/L was significant for treatment failure (19, 20). In our study, with 169 PJI attacks, ESR values at the time of diagnosis were similar in both treatment-responder and non-responder patients; CRP levels were lower in the treatment-responder group, but the difference was insignificant in the multivariate analysis.
In a study evaluating the usability of ESR and CRP before reimplantation in two-stage revision surgery, the sensitivity of CRP was 50%, ESR was 75%, and the combined use of both tests was 100% (21). In another study evaluating treatment response after DAIR, CRP was significantly lower in patients with successful treatment, especially after the fourth week (22). However, some studies show that ESR and CRP monitoring is not beneficial in the postoperative period. In our study, the ESR values at the end of the treatment were significantly lower in the treatment-responder group, and as expected, this difference appeared later due to the longer half-life of the test. More importantly, CRP values were significantly lower in the treatment-responder group beginning from the second week of follow-up, a shorter time than previous studies on this subject. Physicians may prefer to check the ESR and CRP levels less frequently and to test second-week CRP levels to predict treatment response if the patient does not need to come to the hospital and can be monitored by online follow-ups for their symptoms and signs.
One of the main factors affecting the treatment response is choosing the right surgical method for each patient. The success rate of surgical methods changes from center to center; for DAIR, this ranges from 0 to 89% (12, 23). Appropriately selected patients may benefit more from treatment (short duration of symptoms, well-fixed prosthesis with good soft tissue support, and without sinus tract) (24). The interest in one-stage revision has increased in recent years because it is a single operation with a lower cost. Its success rate varies between 77-100%, while the reinfection rate was 7.6% in a review (1, 25). Although one-stage revision may be preferable for appropriate candidates, some study results of two-stage revisions are more promising. Two-stage revision’s success rate was 82-100% in a review evaluating knee PJIs, while in a review evaluating hip arthroplasty, it was 89%, and the reinfection rate was 8.8% (95% CI=7.2-10.6) (25, 26). In a study which evaluated patients who underwent resection surgery, the success rate was 97%, and joint function was satisfactory in 79% of them (27). In our study group, which has a much higher patient number compared to these studies, the success rate was lowest in the DAIR group, whereas it was highest in two-stage revisions. Since our center is a tertiary care referral center for complicated patients and most of our cases were delayed and late, generally, two-stage revisions were chosen, and they were more successful. The treatment success of DAIR may be lower in inappropriate cases such as late infections or unwell-fixed joints, so we may underline that DAIR can cause further harm with additional surgery and therapy needs for unsuitable patients.
A two-stage revision is recommended for patients who had treatment failure after DAIR, resection arthroplasty, or amputation and for those who do not respond or are not suitable for this surgery as a salvage therapy (1, 28). In case of treatment failure after two-stage revision, suppressive antibiotic treatment, DAIR, repeated two-stage revision, resection arthroplasty, arthrodesis, or amputation is recommended (1). In our study, treatment response was 83% in patients who underwent two-stage revision because of DAIR failure.
The antibiotic treatment must be arranged according to the causative microorganism and the surgical procedure applied. Antibiotics with good penetration into the bone and joint tissue, effective on the biofilm layer, and fewer side effects should be chosen (1, 10, 17). Teicoplanin is an important alternative therapy in the treatment of bone and joint infections, but there is limited data on its use in prosthetic joint infections. It has a better safety profile than other glycopeptide antibiotics, has fewer side effects, and fewer interactions with other drugs. Teicoplanin also is infused more quickly, used once daily, and can be applied as OPAT. Teicoplanin is generally used in resistant Gram-positive PJIs or when beta-lactams cannot be used and is also used in empirical treatment (29, 30). In addition to its routine intramuscular or intravenous use, teicoplanin can be administered subcutaneously, three times a week at high doses or as an OPAT (31). Therapeutic drug monitoring is recommended (32).
In a multicenter study examining patients who underwent OPAT for bone and joint infections in Italy, teicoplanin (38%) and ceftriaxone (14.7%) were the two antibiotics generally chosen. Of those patients, 13.4% were followed up with the diagnosis of PJI, and the failure rate after treatment was found to be 15%. In an older study evaluating the efficacy of teicoplanin in bone and soft tissue infections, treatment success was achieved in 50% of the patients diagnosed with PJI (33, 34). Consistent with the literature, the treatment response rate was higher in patients using teicoplanin for more than two weeks, and it was statistically significant.
Our study has some limitations. Firstly, it has a single-center design and a relatively high rate of culture-negative infections. Furthermore, potential bias in evaluating the efficacy of teicoplanin could have been observed due to its frequent combination with other antibiotics and the absence of detailed information regarding the comparator antibiotics. Nevertheless, it has some strengths, such as the number of patients diagnosed with PJI included is quite high. It evaluates the factors that are effective in both preoperative and postoperative periods for the cure of PJI treatment, the success of treatment methods, and especially the use of teicoplanin in treating PJI, about which studies are limited.
In this retrospective study, we evaluated the effectiveness of surgical and medical treatments in the management of PJIs and the risk factors for treatment failure. The results indicate that preoperative parameters such as Hb, Hct, and CRP levels play a significant role in predicting treatment outcomes, with CRP levels in the postoperative period providing an early indication of response to therapy. Two-stage revision surgery demonstrated the highest success rates among surgical options, while DAIR proved effective in selected cases. Teicoplanin, with its low side effect profile and once-daily dosing, emerged as an effective treatment option for Gram-positive and culture-negative infections. Based on our findings, we recommend a personalized approach tailored to individual patient characteristics for PJI management.