Introduction
Vaccines to prevent SARS-CoV-2 infection are the most promising and effective approach to curb the COVID-19 pandemic, as well as to reduce hospitalizations and prevent mortality (1). In our country, the CoronaVac (Sinovac Biotech, China) vaccine started to be administered as of January 13, 2021, and the Comirnaty (BNT162b2, Pfizer-BioNTech) vaccine as of April 2, 2021, with the approval of the Republic of Turkey Ministry of Health Turkish Medicines and Medical Devices Agency (TITCK) Science Commission (2, 3). Within the scope of COVID-19 vaccination in our country, 56,708,402 people have received one dose of any vaccine, 51,242,632 people two doses, and 15,321,143 people three doses as of December 22, 2021 (4).
Despite the effective COVID-19 vaccine applications in the world and our country and the reported effectiveness of vaccines, unfortunately, many patients needed to be treated in hospital or even died because of severe COVID-19 infection (5). Studies from different countries showed that those with severe COVID-19 were unvaccinated or partially vaccinated (6-8).
The Centers for Disease Control and Prevention (CDC) recommended that all individuals over the age of 12 should get a booster dose, regardless of which COVID-19 vaccine they first received, against severe illness (9). Moderately or severely immunocompromised people may also get a second booster (10). Real-life data after major vaccination profiles show that COVID-19 breakthrough infections, hospitalization, and death differ across vaccination profiles with different shots and types of vaccines (11). Also, CoronaVac vaccinees with significantly reduced neutralizing antibodies may face a higher risk of breakthrough infection (12).
To our knowledge, this is the first study in the literature to evaluate the COVID-19 vaccination status of breakthrough COVID-19 infection inpatients, during the delta variant outbreak, in Turkey, where a unique hybrid vaccination model is implemented. Although COVID-19 vaccines have been administered free of charge to all citizens over the age of 13 by the Ministry of Health of the Republic of Turkey, patients who need hospitalization and intensive care support because of COVID-19 have still been a serious burden on the health system.
In our multi-center point prevalence study, the vaccination status and risk factors of the need for intensive care support of hospitalized breakthrough COVID-19-infected patients, as well as the effectiveness of the vaccination programs carried out by the Republic of Turkey Ministry of Health, were investigated. We aimed to address the following two questions: (1) what risk factors are associated with COVID-19 infection due to VOCs; (2) what is the role of vaccination on SARS-CoV-2-associated severe outcomes among the infected people? We found older age, hypertension, DM, CHF and being partially vaccinated associated with the need for ICU support in breakthrough COVID-19 infections.
Materials and Methods
Study Design
This study was designed by the Adult Immunization Study Group of the Turkish Society of Clinical Microbiology and Infectious Diseases (KLİMİK), as a point-prevalence study. The study was conducted among hospitalized COVID-19 patients in 19 centers from five different geographical regions of Turkey, on December 22, 2021. Medical centers that responded to the call via e-mail were included in the study.
Inclusion and Exclusion Criteria
Patients with SARS-CoV-2 PCR test positivity in the nasopharynx or lower respiratory tract samples and those hospitalized in COVID-19 wards or intensive care units (ICUs) on the study day constructed the study population. All patients admitted to the ward or ICU and followed for more than 24 hours in the participating hospitals and patients who were in the ward at 8.00 a.m. and were not discharged until the time of the survey were included in the study. Patients under the age of 18 and outpatients were excluded.
Data Collection
The database in Microsoft Excel (Microsoft Corp., USA) format containing the necessary data for the study, which all the researchers should collect, was created by the principal investigator. This database was shared with the researchers from participating hospitals via e-mail and revised according to the feedback. Information including patient’s age, gender, comorbidities, drug usage, COVID-19 vaccination history, symptoms (such as fever, cough, and dyspnea) and clinical findings (such as tachypnea), treatments (such as oxygen support, high flow oxygen therapy, and invasive or non-invasive mechanical ventilation), laboratory and radiological findings were collected.
Definitions
Patients were divided into two groups as ‘fully’ and ‘partially’ vaccinated according to CDC definition criteria (11) for the Comirnaty vaccine and the Ministry of Health’s criteria for CoronaVac (12).
Patients meeting all of the following criteria were defined as ‘fully vaccinated’:
- At least two doses of inactivated (CoronaVac) or mRNA vaccine (Comirnaty),
- At least three doses of any COVID-19 vaccine for immunosuppressed patients,
- At least 14 days after receiving the last dose of the vaccine,
- ≤90 days after the last dose of inactivated vaccine (CoronaVac) or ≤150 days after the last dose of mRNA vaccine (Comirnaty).
- All the other patients were defined as ‘partially vaccinated’.
Stem cell or solid organ transplant recipients, chronic kidney disease or hemodialysis patients, HIV-infected patients, patients receiving active chemotherapy or radiotherapy, and patients using immunosuppressive drugs (biological agents and immunosuppressive doses of corticosteroids) were defined as patients having the immunosuppressive condition.
The diagnosis of COVID-19 infection was made based on SARS-CoV-2 molecular test positivity. Asymptomatic, mild, moderate, severe, and critical COVID-19 infections were defined according to the National Institute of Health (NIH) COVID-19 treatment guidelines (13). Asymptomatic patients were not included in the analysis.
Outcome Measures
The primary outcomes of the study were to determine the COVID-19 vaccination rate, the type of vaccine administered, the number of vaccine doses, and the time from the last vaccine dose to the diagnosis of breakthrough infection in hospitalized COVID-19 patients. The secondary aim of the study was to determine the risk factors of the need for ICU support.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) for Mac OS X 25.0 (IBM Corp., Armonk, NY, USA). The normal distribution of the data was determined by the Shapiro-Wilk test, histogram, and Q-Q plots. The categorical variables were analyzed with a Chi-square test and presented as frequency and percentage. For continuous variables, mean values and standard deviation (SD), or median values and an interquartile range (IQR) of 25%-75% were presented. The non-parametric values were analyzed using the Mann-Whitney U test. To determine risk factors for ICU support, such as age, hypertension, diabetes mellitus (DM), coronary artery disease, congestive heart failure (CHF), malignancy, cerebrovascular disease, and vaccination history, multivariate models included parameters with a p-value of < 0.2 in univariate analysis. The statistical significance was set as p<0.05.
Results
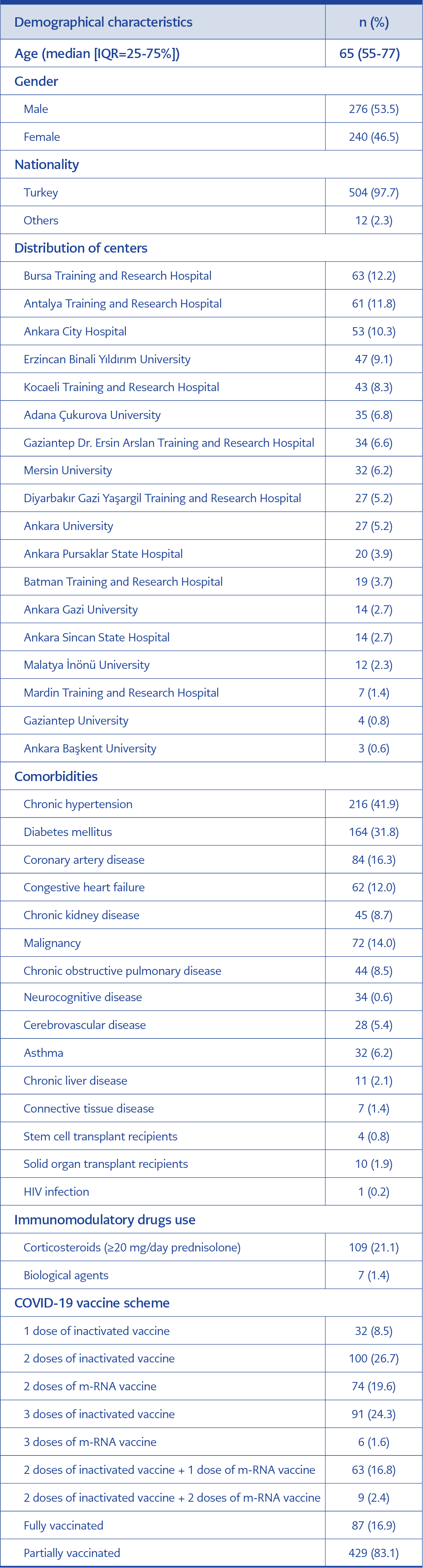
Table 1. Demographical characteristics of patients (n=516).
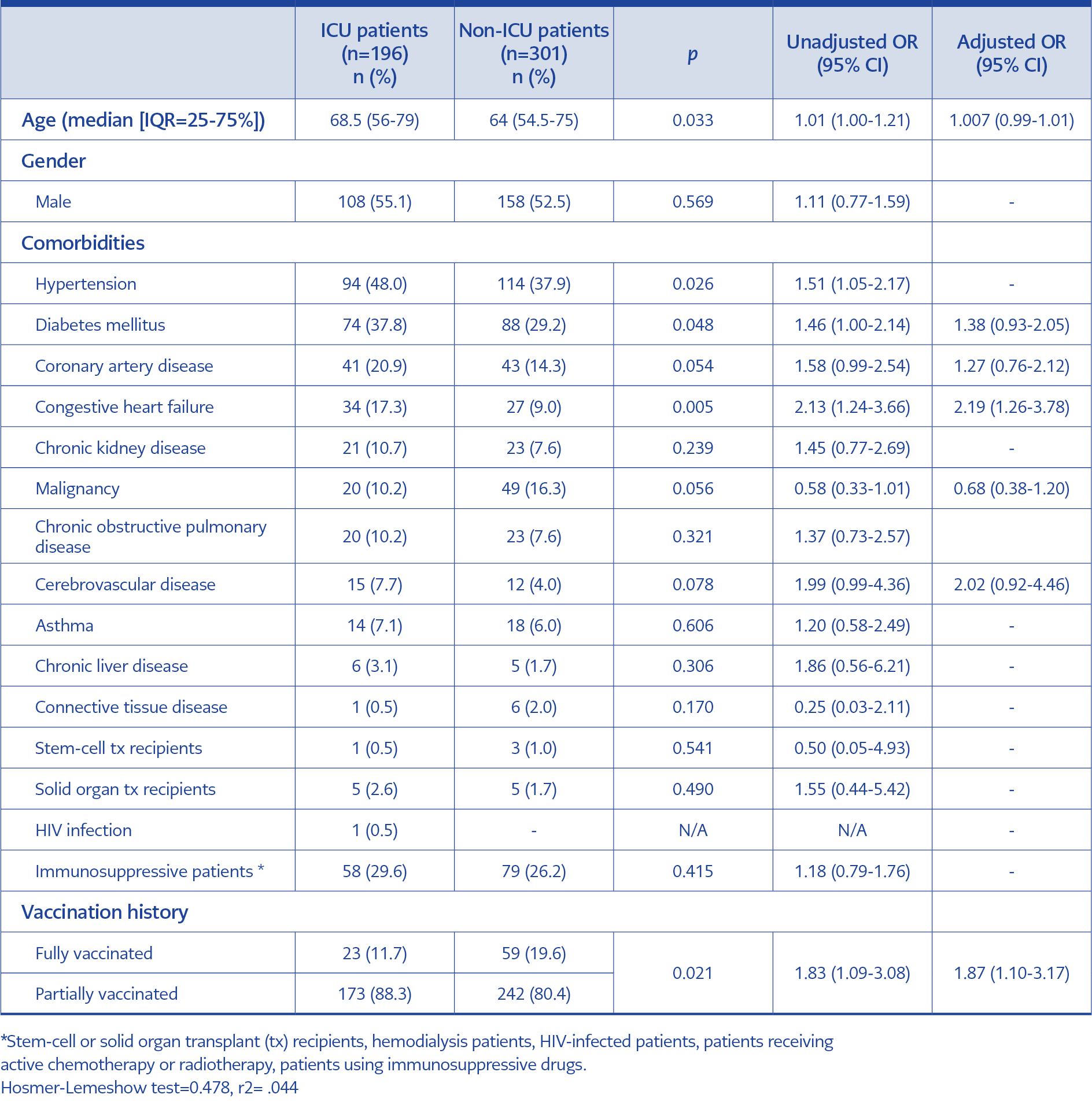
Table 2. Comparison of patients’ demographical characteristics, comorbidities, and vaccination status according to ICU admission (n=497).
A total of 516 patients were included in the study. Demographical characteristics, comorbidities, and vaccination status were evaluated and presented in Table 1.
The median time between the last dose of vaccine and SARS-CoV-2 PCR positivity was 139 (IQR=25-75%; 99-180) days.
Patients were grouped as ICU (n=197) and non-ICU (n=319). Demographical characteristics, comorbidities, and vaccination status were compared between the groups. Nineteen patients hospitalized due to COVID-19-unrelated conditions were excluded from the analyses (Table 2).
Discussion
Because of the rapidly changing nature of the COVID-19 pandemic, countries need to analyze real-life data constantly and shape their vaccine strategies dynamically. Especially in susceptible populations, identifying risk factors for breakthrough infections and intensive care needs is critical. In our study, older age, hypertension, DM, CHF, and being partially vaccinated were associated with the need for ICU support in breakthrough COVID-19 infections. Vaccination status was the primary determinant of the need for ICU support. The need for ICU support was statistically significantly lower in the fully vaccinated group (p=0.021).
In our country, besides mRNA vaccines, the inactivated vaccine is also being used within the scope of COVID-19 vaccination, and vaccine preference is free. Due to this hybrid vaccination model, heterogeneous vaccinated groups emerge. The susceptibility of the person with each vaccination schedule to COVID-19 infection also differs. Previous studies show that mRNA vaccines reduce mortality in people infected with COVID-19. Male gender, immunocompromised status, and prolonged time after the last vaccine dose were associated with increased risk for breakthrough COVID-19 infection in the patients vaccinated with mRNA vaccines (14). In a meta-analysis investigating the short-term effectiveness of vaccines for preventing hospitalization and death because of the delta variant, two doses of the CoronaVac vaccine had the worst protection rates among all authorized vaccines (15). We know that neutralizing antibody levels potentially correlate with protection against SARS-CoV-2 infections (16), and the CoronaVac neutralizing antibody titers were reported to be short-lived (17). Higher rates of COVID-19 infections are expected due to variants of concern (VOCs) if vaccines with lower efficacy are used (18). In our study, we examined that the most common vaccine scheme in patients requiring hospitalization was three doses of inactivated vaccine, while few patients belonged to the three doses of mRNA vaccine group.
A recent study conducted on patients with emergency department admission because of SARS-CoV-2 infection demonstrated in multivariate logistic regression analysis that age, male gender, presence of at least one comorbid disease, and vaccination status were associated with mortality (19). We performed a one-day point prevalence assessment in our study, so we could not determine the factors affecting mortality, but we determined the factors affecting the need for ICU support.
We evaluated a retrospective cohort of 110,760 US veterans who received primary COVID-19 vaccination series, as well as a subset with an additional booster vaccine, and developed laboratory-confirmed SARS-CoV-2 infection between December 2020 and February 2022. The results showed that older age was strongly associated with severe breakthrough infection. Immunocompromising medications and conditions, chronic comorbid conditions like chronic kidney disease, heart failure, and dementia also were associated with increased risk. Receiving a booster dose was found to be associated with a 50% lower risk of severe breakthrough infection (20). All these findings show similarities with our study. The analysis of this study included infections that occurred during both the delta period (n=29,000) and the omicron period (n=78,000). The numbers of severe breakthrough infections and hospitalizations were equivalent in both periods—736 during delta and 728 during omicron—despite the much larger number of omicron infections overall, supporting the previously recognized lower disease severity of omicron vs. delta in this very large database. According to all these, the severity of breakthrough COVID-19 infection despite vaccination was associated with age, comorbid conditions, immune status, vaccination status of the patients, and VOCs. By evaluating these findings for both studies, we consider that clinical decision-making about patients for booster vaccination will be beneficial.
Coronavirus VOCs (September 2020 UK alpha variant [B.1.1.7], December 2020 South Africa beta variant [B.1.351], May 2021 India delta variant [B.1.617.2], August 2021 Colombia mu variant, November 2021 South Africa-Botswana omicron variant [B.1.1.529]) have had their origins and quickly spread all over the World (18). Studies were conducted to confirm vaccine breakthrough infections with SARS-CoV-2 variants using genome sequencing and to investigate clinical characteristics, especially due to delta and omicron variants (7, 21-24). In our country, SARS-CoV-2 variant analysis was carried out only in the reference laboratory, and only selected samples from all laboratories where SARS-CoV-2 PCR was performed were sent to the reference laboratory as part of surveillance. In line with the sequence analyses studied in reference laboratories, the predominant variant was delta in the period of December 2021, when the study was carried out (25, 26).
Real-world data comparing mRNA and inactivated (CoronaVac) vaccines’ homologous and heterologous boosting are lacking. The results of a retrospective study that evaluated the rate and outcome of COVID-19 in healthcare workers with various vaccination regimens during the omicron BA.2.2 outbreak in Hong Kong showed that using two-dose Comirnaty as a reference, two-dose CoronaVac recipients had a significantly higher risk of being infected (HR=1.69, p<0.0001). Three-dose Comirnaty (HR=0.4778, p<0.0001) and two-dose CoronaVac + Comirnaty booster (HR=0.4862, p=0.0157) were associated with a lower risk of infection (27, 28).
Our study has some limitations. We performed a one-day point prevalence assessment in only hospitalized patients, so we could not determine the factors affecting mortality, and also, our study did not evaluate the vaccine efficacy. The different patient populations in various geographic distributions, different virus circulation dynamics, and different types of healthcare organizations could confound the results. We conducted the study in the centers that responded to our invitation via e-mail, so even though 19 centers were involved, this study could not represent the whole population.
Along with the possible emergence of various SARS-CoV-2 variants in the future, there is a predictable challenge to develop targeted vaccines against mutations on the S protein and terminate the COVID-19 pandemic as soon as possible. Therefore, continuous monitoring of post-vaccination breakthrough infections should be performed by all countries in order to determine the national booster vaccine administration approach which will provide the highest protection to vulnerable individuals. Therefore, the real-life data of our study may guide the plans of national vaccine strategies on who may optimally benefit from a booster COVID-19 vaccination.