Introduction
Tuberculosis (TB) is a common disease with high mortality and morbidity worldwide. Globally, an estimated 10.6 million people (95% uncertainty interval [UI]=9.9-11.4 million) developed TB in 2022, compared with 10.3 million in 2021 and 10.0 million in 2020. TB caused an estimated 1.30 million deaths worldwide in 2022 (95% UI=1.18-1.43 million). This was down from best estimates of 1.4 million in both 2020 and 2021 and almost back to the level seen in 2019 (1).
The main drugs used to treat Mycobacterium tuberculosis complex (MTC) are isoniazid (INH), rifampicin (RIF), ethambutol (EMB) and streptomycin (SM). Different levels of resistance to these drugs are developing, and cases resistant to INH and RIF are called multidrug-resistant TB (MDR-TB). The burden of drug-resistant TB (DR-TB) is also estimated to have increased between 2020 and 2021: in 2022, 73% (2.9/4.0 million) of people diagnosed with bacteriologically confirmed pulmonary TB were tested for RIF resistance (RR-TB), up from 69% (2.4/3.5 million) in 2021 (1, 2).
Methods used to identify Mycobacterium spp. include the detection of acid-resistant bacilli (ARB) by smear microscopy, growth in solid or liquid media, and molecular and biochemical tests. Although classic diagnostic methods remain important, BD BACTEC™ MGIT™ 960 identification system (Becton Dickinson, USA) and Mycolor TK® automated mycobacterial culture system (TIBO Trends in Innovative Biotechnology Organization, İstanbul, Türkiye) are the automated diagnostic methods used to produce, identify the factor and determine drug susceptibility (3). This study aimed to determine the growth rates and drug susceptibility levels of patients with MTC growth in cultures obtained in our hospital over a period of 3.5 years and compare the results with those found in our country and other countries. It also aimed to evaluate the results of supplementing classical methods such as Lowenstein-Jensen (LJ) with liquid TK MEDIUM® (TIBO Trends in Innovative Biotechnology Organization, İstanbul, Türkiye) and to determine the relationship between the growth rates obtained with both methods.
Materials and Methods
In our study, we retrospectively reviewed the results of specimens (such as sputum, bronchial lavage, and abscess) collected from patients who were evaluated with a presumptive diagnosis of TB and sent to the microbiology laboratory of Sivas Numune Hospital. Susceptibility to the main drugs used to treat TB (SM, INH, RIF, and EMB) was assessed in patients who were ARB-positive or negative and had MTC growth in culture.
The samples sent to the laboratory had undergone homogenization and decontamination procedures, with the exception of sterile fluids (such as cerebrospinal and pleural fluids), 0.5 mL of each sample was seeded simultaneously on TK medium and LJ medium (Salubris, Türkiye) on the basis of color change. TB identification and antimicrobial susceptibility testing were performed using the TK ANTI-TB and PNB KIT® (TIBO Trends in Innovative Biotechnology Organization, İstanbul, Türkiye) in the Mycolor TK® mycobacterial culture system (TIBO Trends in Innovative Biotechnology Organization, İstanbul, Türkiye) according to the manufacturer’s operating procedures. (3). TK ANTI TB & PNB KIT® includes TK MEDIUM® with major antituberculosis drugs (pyrazinamide, RIF, EMB, and SM) required for both differentiation of MTC from non-tuberculous mycobacteria and for anti-TB susceptibility testing. TK PNB® is a type of TK MEDIUM® containing para-nitrobenzoic acid (750 μg/mL).
Cultures inoculated on TK MEDIUM® were incubated in the Mycolor TK® mycobacterial culture system, and cultures inoculated on LJ were incubated in an oven at 37°C for 6-8 weeks. After ARB staining, blood agar and EMB cultures were added to the patient samples showing growth signals in the Mycolor TK® automated system; growth in TK MEDIUM® and absence of growth in PNB KIT® were considered in favour of MTC and were added to tubes containing antimycobacterial drugs. Those showing a growth signal in the PNB KIT® were interpreted in favour of an atypical mycobacterium. When the TK MEDIUM® tube of a strain turned yellow, the strain was reported as resistant to the antimycobacterial drug in the tubes containing antimycobacterial drugs and as susceptible to the antimycobacterial in the red tubes (4). In the antibiotic susceptibility test in the automated incubator, those below the growth signal line were considered susceptible, and those above the line were considered resistant. In addition, patients who were ARB-positive, culture-negative, and citizens and non-citizens of the Türkiye were retrospectively examined from the laboratory records. Only one growth of the same patient within one year was included in the study.
The data obtained from our study were loaded into the SPSS program (version 22.0). When parametric test assumptions were met, the significance test of the difference between two means in independent groups was used (Kolmogorov-Smirnov). When parametric test assumptions were not met, the Mann-Whitney U test and chi-square test were used. The margin of error was expressed as 0.05. Approval was obtained from the Ethics Committee of Sivas Cumhuriyet University with decision number 2016-04/09.
Results
The results of specimens collected from a total of 3720 patients who were evaluated with a presumptive diagnosis of TB were retrospectively reviewed, and the drug susceptibility testing of 74 patients with MTC growth in culture was included in the study. The mean age of the patients was 43.41±20.997 years, and there was no difference between the sexes (p>0.05). Susceptibility and resistance of the samples to INH, RIF, EMB and SM, which are the primary anti-TB drugs, were investigated. While a total of 104 patients were found to be ARB-positive, 5 ARB-positive patients had atypical mycobacteria, and the number of ARB-negative culture-positive patients was 25 (33.7%).
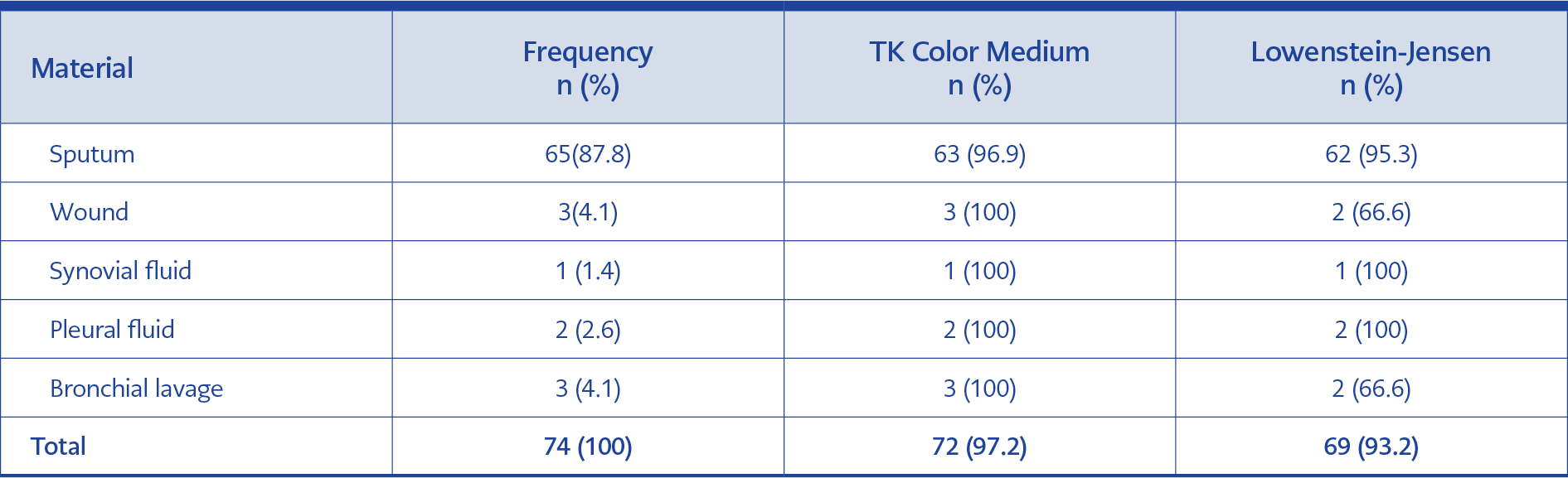
Table 1. Growth rates of patient samples in culture media.
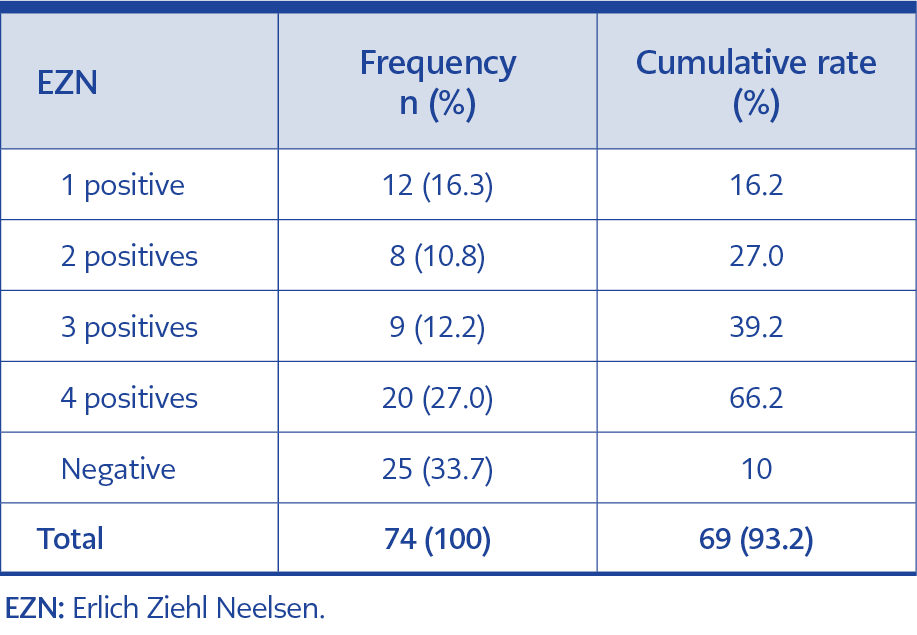
Table 2. EZN positivity rates for patient samples in the culture media.
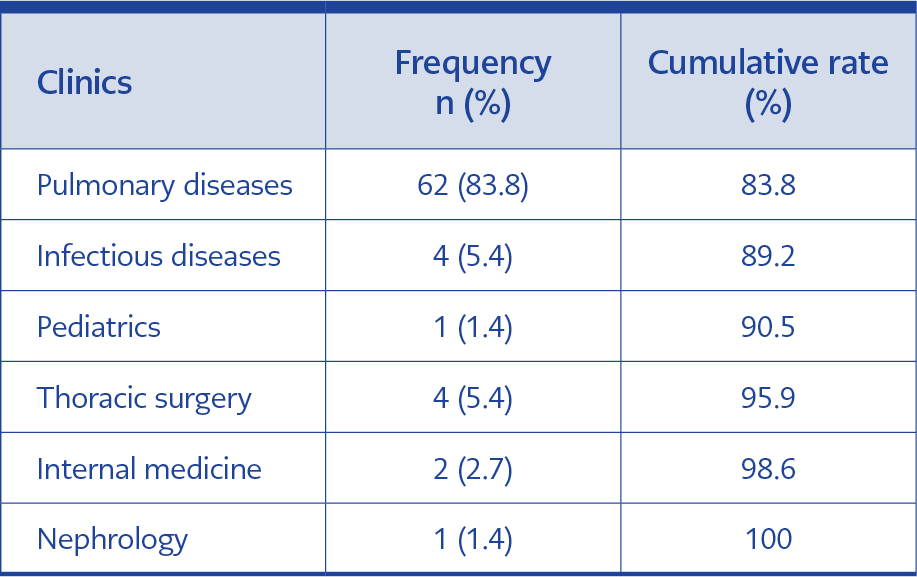
Table 3. Distribution of culture-positive samples according to clinics.
The sputum sample was the most frequently sent material, with a rate of 87.8% (n=65) (Table 1). In the ARB 4-positive endoscopic material, no growth was detected in either TK MEDIUM® or LJ medium. The rate of patients with MTC growth in the ARB-negative culture was 33.7% (n=25) (Table 2). Of the patients, 83.8% were followed up in the thoracic service, 5.4% in the infectious disease service, 1.4% in the pediatric service, 5.4% in the thoracic surgery service, 2.7% in the internal medicine service and 1.4% in the nephrology service (Table 3). Four of the 74 culture-positive specimens belonged to patients of foreign nationalities living in our country (5.4%). None of the foreign patients showed resistance to any of the drugs. One wound material from a foreign patient was found to be ARB-positive, but no growth was observed in culture in both TK and LJ media.
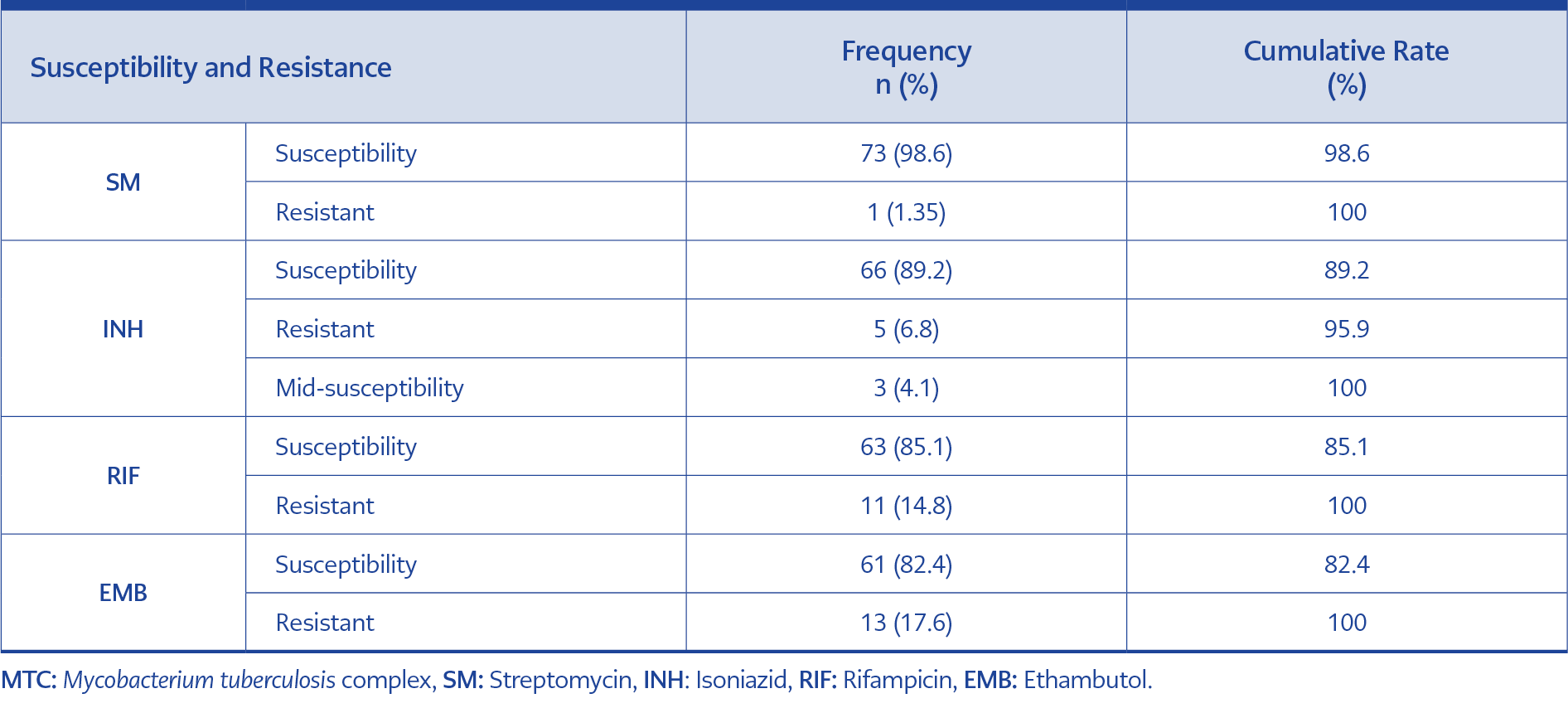
Table 4a. Drug susceptibility and resistance status of MTC isolates grown in cultures.
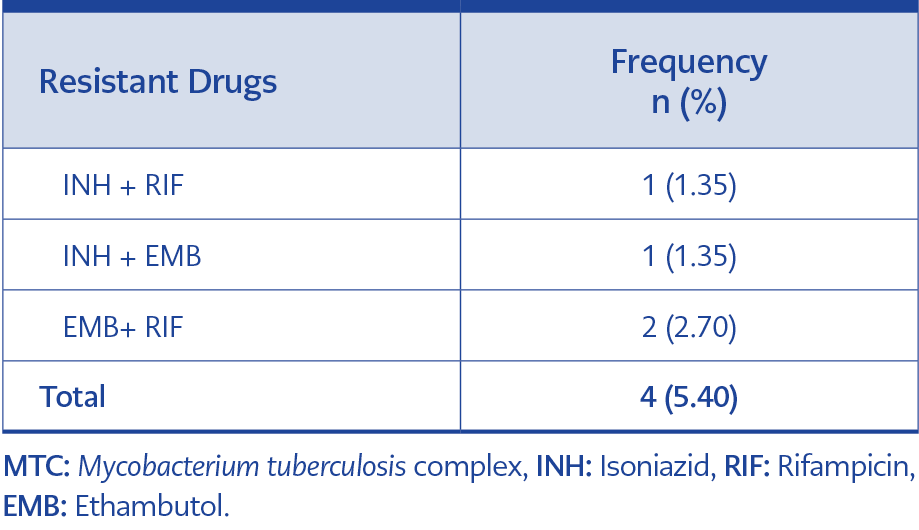
Table 4b. Multiple drug-resistance rates of MTC isolates (n=77).
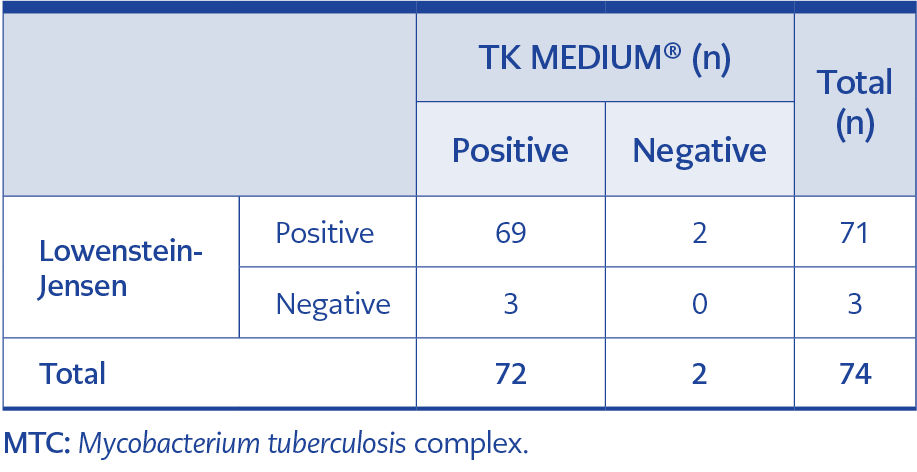
Table 5. Distribution of the MTC isolates based on their production medium (n=74).
The rate of INH+RIF-resistant patients was 1.35% (n=1). Two-drug resistance was detected as 5.4%. The rate of single-drug resistance to INH was 6.8%, 4.1% were moderately susceptible. The rate of samples resistant to RIF was 14.8%, to EMB was 17.6%, and to SM was 1.35% (Table 4a, 4b). The isolates sent to the laboratory were inoculated simultaneously on LJ and TK MEDIUM®. While a faster reproductive signal was observed in the medium in the automated system, there was no significant difference between the two systems in terms of positivity (p>0.05) (Table 5).
Discussion
The Sustainable Development Goals for 2030 were adopted by the United Nations in 2015 to fight TB. One of the goals is to end the global TB epidemic. The target for 2050 is to eliminate TB, i.e. to reduce the number of cases to less than one in a million. Achieving these goals will require appropriate health policies, personalized care, and regular treatment for every TB patient. For MTC, one of the world’s oldest fatal diseases, the development of resistance to treatment is another notable problem, despite the fact that it has been completely treatable for 50 years. (5, 6).
The World Health Organization (WHO) has been tracking TB and its drug resistance for many years. Thirty high-burden countries accounted for 87% of the world’s TB cases in 2022. Two-thirds of the global total was in eight countries: India (27%), Indonesia (10%), China (7.1%), the Philippines (7.0%), Pakistan (5.7%), Nigeria (4.5%), Bangladesh (3.6%) and the Democratic Republic of Congo (3.0%) (1). The incidence calculated according to the number of registered cases in our country is 13.5 per 100,000 in 2019 and 10.6 per 100,000 in 2020. The total case rate was 13.7 per 100,000 in 2019 and 10.7 per 100,000 in 2020, with a decrease of 22.1% in 2020 compared to 2019. This unexpected decrease was evaluated as a reflection of the COVID-19 pandemic (7).
In 2019, the three provinces with the highest number of cases were İstanbul (n= 3392), İzmir (n=612) and Ankara (n=591), while the three provinces with the lowest number of cases were Ardahan (n=3), Tunceli (n=3) and Gümüşhane (n=6). In 2020, the three provinces with the highest number of cases were İstanbul (n=2838), Ankara (n=460) and Bursa (n=451), while the three provinces with the lowest number of cases were Ardahan (n=4), Tunceli (n=4) and Bayburt (n=7). When total case rates by provinces are evaluated, the three provinces with the highest case rates in 2019 were Edirne (24.9 per 100,000), İstanbul (21.9) and Sakarya (20.7), respectively. Ardahan (3.1), Tunceli (3.5) and Gümüşhane (3.6) have the lowest case rates. In 2020, Karabük (23.4), Istanbul (18.4) and Çanakkale and Kırklareli (17.4) were the three provinces with the highest case rates, while Niğde (3.9), Ardahan and Van (4.2) and Uşak (4.3) are the provinces with the lowest case rates (7). It is important to note that the geopolitical position of our country is on the transition path between Asia and Europe, receiving immigrants from Asian countries (such as Afghanistan and Syria). Although TB is a preventable disease, there are cases that are resistant to treatment and lead to death. In our retrospective study, 4 out of 74 (5.4%) culture-positive patients were from foreign nationalities who came from countries such as Pakistan and Afghanistan. None of the samples from these patients was drug-resistant.
The WHO uses five categories to classify cases of DR-TB: isoniazid-resistant TB; RR-TB and MDR-TB; extensively DR-TB (XDR-TB); and pre-XDR-TB. Pre-XDR-TB is TB that is resistant to RIF and any fluoroquinolone (a class of second-line anti-TB drug). XDR-TB is TB resistant to RIF, plus any fluoroquinolone, plus at least one of either bedaquiline or linezolid. Globally in 2022, 73% of people (2.9/4.0 million) diagnosed with bacteriologically confirmed pulmonary TB were tested for RIF resistance. Among those tested, 149,511 people with MDR/RR-TB and 27,075 people with pre-XDR-TB or XDR-TB were detected, totalling 176,586 (4.4% of those tested). India, the Philippines and the Russian Federation account for 42% of the cases (1).
In our country, according to the Ministry of Health’s Tuberculosis Control Department 2021 Report, in 2019 the most common single drug resistance was INH (5.4%) and SM (4.8%), dual drug resistance was INH-SM (2.4%) and triple drug resistance was INH-RIF-SM (0.7%). The overall drug resistance rate was 16.7% among patients who underwent drug resistance testing. The rate of MDR-MTC was 1.8% (n=93) in new cases and 9.1% (n=34) in previously treated cases. In 2020, the most common single drug resistance was INH (5.0%) and SM (4.5%), dual drug resistance was INH-SM (2.0%) and triple drug resistance was INH-RM-SM (0.6%). The overall drug resistance rate was 16.3% among patients who underwent drug resistance testing. The rate of MDR-MTC was 2.2% (n=88) in new cases and 8.6% (n=25) in previously treated cases (7).
In the resistance study which was conducted in our country by Aydın et al., the single drug resistance to INH was found to be at 6.1%, to RIF at 0.5%, to SM at 5.2%, and to EMB at 2.4%; the rate of the multiple drug resistant M. tuberculosis complex resistant to INH and RIF was at least 4.8% (8). The MDR TB rates vary between 2.2% and 14.7% in the resistance studies conducted in various regions of Türkiye. Öz et al. reported resistance rates of 14.4% for INH, 7% for RIF, 2.1% for SM and 2.8% for EMB among the tested anti-TB drugs and found the MDR-MTC rate to be 4.6% (9). In their study conducted in Sivas province between 2005 and 2010, Çelik et al. found the MDR-MTC rate to be 1.1%, and while the highest resistance was observed at a rate of 3.7% to INH and 3.7% to SM, resistance to RIF and EMB was observed at lower rates as 1.1% and 0.5%, respectively (10). They found multiple drug resistance in 6.9% of the strains tested (10). In our study, the rate of MDR-MTC resistance was 1.35% (n=1). We found two-drug resistance at 5.4%. The rate of single-drug resistance to INH was 6.8%, and 4.1% were moderately susceptible. The rate of samples resistant to RIF was 14.8%, to EMB was 17.6%, and to SM was 1.35% in our study.
The WHO recommends using the liquid medium for M. tuberculosis culture (11). In the reciprocal study carried out by Somoskovi et al. in solid and liquid media, 93% of the mycobacterial strains isolated were found in the BACTEC medium and 80.7% in the LJ medium (12). In their study of sterile body fluids from 214 patients suspected of having extrapulmonary TB, Wang et al. found the rate of samples positive in at least one of the Myco/F lytic, MGIT 960 and LJ systems to be 48.13% (n=103) and determined 86.41%, 75.73% and 43.72% positivity, respectively, in samples classified as MTC (Capilia TB-Neo Assay) (13). They found the superiority of growth in liquid culture systems to be statistically significant compared to the solid method (p <0.001). Günal et al. reported that only one of the 39 samples with growth in the LJ medium did not grow in the MGIT system (14). In the study by Kurtoğlu et al., eight of the 55 samples with growth in the LJ medium showed no growth in the MGIT medium, and eight of the 55 samples with growth in the MGIT medium showed a negative result in the LJ medium. In our study, three of the 69 samples with growth in the LJ medium did not grow in the TK MEDIUM®, and two of the 71 samples with growth in the TK MEDIUM® gave a negative result in the LJ medium. Therefore, there was no statistically significant difference between the LJ and TK MEDIUM® in terms of mycobacteria production (p >0.05) (14, 15).
TK MEDIUM® (SALUBRIS, Woburn, MA, USA) is a ready-to-use, biphasic, rapid mycobacterial culture medium that provides early detection of mycobacterial growth by changing the color of the medium and does not require the addition of selective antimicrobials. Multiple color indicators are chemically produced and the change in color of the TK medium from the original red to yellow, depending on the metabolites and enzymes produced by the mycobacteria, indicates growth. In addition to differentiating between M. tuberculosis and atypical mycobacteria, in the presence of bacteria or fungi other than mycobacteria, the color changes from red to green to differentiate contamination. One of the advantages is that growth takes a shorter time (7-15 days) compared to LJ. As growth in the TK MEDIUM is detected by color change, it can be easily monitored by visual assessment and can be used in laboratories with standard 37°C incubators (16).
In the study by Kocagöz et al., 16,303 clinical specimens were cultured on TK selective and LJ media over a period of one year; while LJ isolated mycobacteria from 1920 (11.69%) of all specimens, TK SLC isolated mycobacteria from 2070 (12.63%). This result is consistent with the result we obtained in our study, which shows that growth rates in both media were similar. Growth time detection modes were determined to be 12 and 25 days for TK SLC and LJ, respectively, and it was concluded that the TK rapid mycobacterial culture system is a practical and reliable automated system that reduces the time required for both culture and susceptibility results. It supports the conclusion that the TK rapid mycobacterial culture system is a practical and reliable automated system that reduces the time required for both culture and susceptibility results. It also supports the susceptibility rates we obtained in our study, which are similar to the results of other studies (15). There is one study in the literature that evaluated the efficiency of using TK SLC-L (Salubris Inc.) for primary isolation of mycobacteria from clinical specimens by comparing it with the BD BACTEC™ MGIT™ 960 identification system (Becton Dickinson, USA), and it found that the TK SLC-L and MGIT systems had similar percentages of culture positivity (24.0 and 23.3%, respectively). It supports the conclusion that Mycolor TK® can be used efficiently for TB diagnosis in both detailed and resource-limited laboratories, which we advocate based on our study results (17).
In conclusion, we found that the drug resistance rates we obtained in patients with suspected TB who applied to our hospital were similar to the data of the Turkish Ministry of Health and other studies conducted in our country. Our study, which was conducted with liquid and solid media found no difference in the detection of TB bacilli regarding media. Therefore, the liquid media can be effectively used to diagnose TB in resource-limited laboratories because it is ready-to-use, saves time and effort, reduces contamination during testing and facilitates the detection of mycobacterial growth and contamination. Based on these results, we believe that Mycolor TK®, which is manufactured in Turkey, can enable rapid mycobacterial culture in laboratories with limited resources. Further studies should support the efficiency of the liquid automation system used in this study.