Introduction
The most common and serious complication of central venous catheter usage is central line–associated bloodstream infections (CLABSIs) in children and adults (1). Between 2011 and 2014, CLABSIs were the most frequently reported healthcare-associated illness among hospitals in the USA (2). Bloodstream infections associated with central lines are the most significant complications of central venous access devices and increase morbidity, mortality, hospital length of stay, and hospital expenses (2-5).
The International Society for Infectious Diseases (ISID), the Infectious Diseases Society of America (IDSA), and the Infusion Nurse Society (INS) recommended using single-use prefilled flushing syringes (PFSs) to flush the catheter and use needle-free connectors (NFCs) in place of three-way stopcocks (6, 7). Previous research from our institution showed that the use of PFSs and central line bundles, which substitute NFCs for 3-way stopcocks, was linked to a noteworthy drop in the rates of CLABSI in the pediatric intensive care unit (PICU) (8-10).
In 2023, we faced a three-month shortage of the medicinal supplies needed to prevent CLABSI. In this study, we aimed to present our experience with the raised CLABSI rates at the PICU during the NFC and PFS shortage in this study.
Materials and Methods
This retrospective study was carried out at a tertiary training hospital from January 1, 2023, to December 31, 2023. Starting in June 2013, our hospital implemented a central line bundle that included the following measures: ultrasonography during insertion, strict hand hygiene, aseptic skin preparation (2% chlorhexidine in 70% alcohol solution), and barrier precautions (mask, gown, protective eyewear, cap, sterile gloves). During maintenance, we additionally used BD Q-SyteTM needle-free connectors (Becton, Dickinson and Company, USA), daily catheter site and cap connection evaluations, and BD PosiFlushTM NaCl 0.9% 10-mL sterile single-use prefilled syringes (Becton, Dickinson and Company, USA).
CLABSI was proven when bacteremia or fungemia was found in a patient with a central venous catheter for more than 48 hours, multiple positive blood cultures from a peripheral vein, and clinical indications of infection.
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 20.0 (IBM Corp., Armonk, NY, USA). The Poisson 95% confidence interval (CI) was used to compute the daily count of CLABSI for each time period and the relative risk reduction across groups, which was expressed as a percentage. In order to compare the risks for each of the two groups with a 95% CI for the incidence rate, the relative risk ratio was also computed using MedCalc 11.6 software (MedCalc Software Ltd, Belgium). The statistical significance was set as p<0.05.
The Ethics Committee of Dr. Behçet Uz Children’s Diseases and Surgery Training and Research Hospital approved the study on March 28, 2024, with decision number GOA-27/28.03.2024.
Results
A total of 32 patients with CLABSI included 19 (59.4%) males and 13 (40.6%) females. With a range of 4 months to 17 years, the patient’s median age was 15 months. Of the patients, 28 (87.5%) had an underlying disease and, 4 (12.5%) had no underlying condition. The prevalent underlying illnesses included congenital heart disease (n=4, 12.5%), cerebral palsy (n=4, 12.5 %), spinal muscular atrophy (n=3, 9.4%), neuro-metabolic diseases (n=15, 46.9%), and pediatric cancer (n=2, 6.3%). The most frequent causes of hospitalization in the PICU were heart failure (n=3, 9.4%), renal failure (n=2, 6.3%), sepsis and septic shock (n=6, 18.8%), pneumonia (n=15, 46.9%), and status epilepticus (n=6, 18.8%). Of the patients, 96% (n=29) had a nasogastric tube, 93.4% (n=30) had urine catheters, and 84.4% (n=25) were on mechanical breathing. Additionally, whole parenteral feeding was used by 56.3% (n=18).
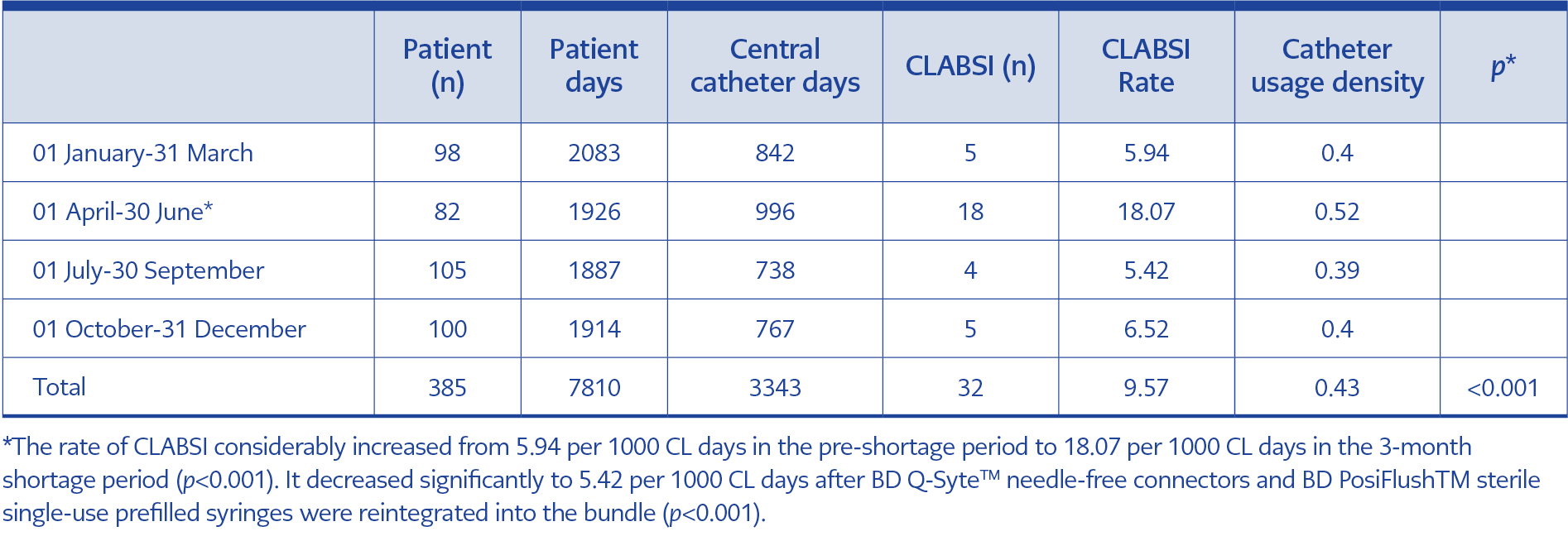
Table 1. Three monthly analyses, including patient counts, patient days, central catheter days, CLABSI number, CLABSI rate and catheter usage density.
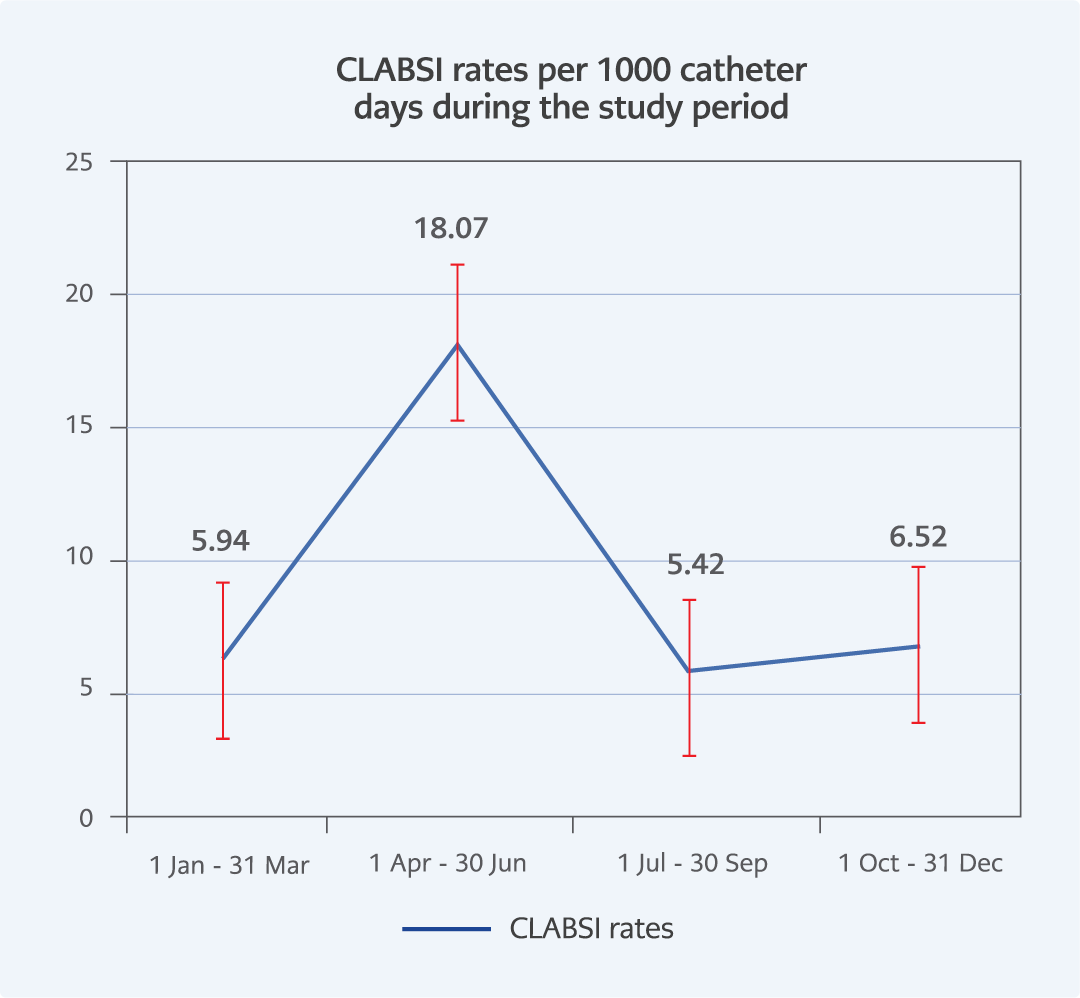
Figure 1. The rate of CLABSI increased between the period of 01 April to 30 June 2024.
There were 385 patients overall in 2023-2024 and 7810 patient days. Table 1 shows 3343 catheter line days in total; 32 CLABSIs were recorded, equivalent to an overall rate of 8.57 CLABSIs per 1000 CL days. The CLABSI rate for three months was as follows: 5.94 per 1000 CL days between January-March, 18.07 per 1000 CL days between April-June, 5.42 per 1000 CL-days between July-September and 6.52 per 1000 CL days between October-December. During the three-month shortage period, the rate of CLABSI increased dramatically from 5.94 per 1000 CL days to 18.07 per 1000 CL days. After BD Q-SyteTM needle-free connectors (Becton, Dickinson and Company, USA) and BD PosiFlushTM sterile single-use prefilled syringes (Becton, Dickinson and Company, USA) were reintegrated into our practice, the incidence of CLABSI significantly fell to 5.42 per 1000 CL days (p<0.001) (Table 1, Figure 1).
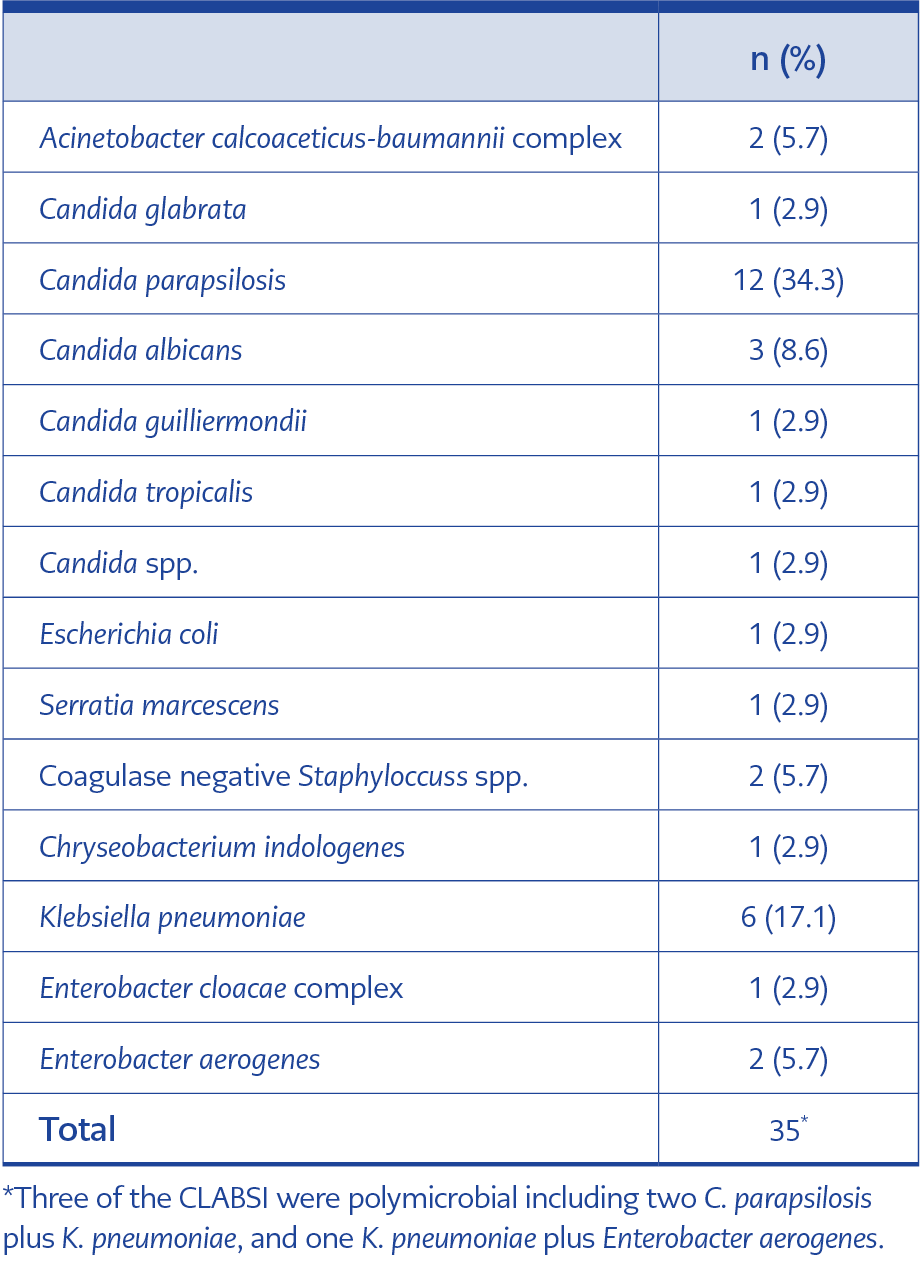
Table 2. The microbiological distribution of causative agents of CLABSI.
Microorganisms with a single origin caused 29 (90.7%) CLABSIs, and polymicrobial pathogens caused 3 (9.3%). Klebsiella pneumoniae (17.1%, n=6) and Candida parapsilosis (34.3%, n=12) were the most frequently isolated microorganisms were. Table 2 shows all species isolated.
Discussion
In this study, the CLABSI rate increased approximately threefold when NFC and PFS were in short supply. It then sharply declined as soon as they were once again available. Our study is one of the few examinations in which the lack of medical devices produced undesirable results.
About one-third of the microorganisms detected in our study were related to C. parapsilosis, the most prevalent microbe. Catheter infections linked to C. parapsilosis have been linked to longer central line days and the ability to form biofilms (11). Biofilms formed by C. parapsilosis can nevertheless form on medical devices such as peripheral venous catheters and central venous catheters, even though reports suggest that the microorganism creates a less complicated biofilm than Candida albicans in terms of both quantitative and structural characteristics (12). Furthermore, because of its tendency to colonize in the hands of medical professionals, C. parapsilosis is a high-risk candidate for catheter infections (13). The most frequently isolated organism causing CLABSIs in the PICU at the same research facility was C. parapsilosis (8). According to additional research from our center, the complete central line bundle successfully reduced the rate of Candida-related central line-associated bloodstream infections, including NFC and PFS (9). Unexpectedly, this indicated that the shortage of medical supplies led to an increase in the rate of CLABSIs caused by C. parapsilosis.
When demand outpaces supply, it is referred to as a shortage event and can impact both medical services and devices (14). The temporary suspension and distribution of dehydrated alcohol in the United States from April to September 2011 led to a change in the dosage and use of ethanol for the prevention of catheter infections. Ralls et al. hypothesized that a decrease in ethanol use led to a rise in catheter infections (15). Furthermore, a recent multicenter survey found that 58% of the centers anticipated higher CLABSI during ethanol storage (16).
This experience demonstrated the significance of maintaining medical devices for a successful central line prevention program, even though it was not the same device. A study conducted at our center from 2007 to 2020 found that the CLABSI rate dropped from 10.5 to 3.6 per 1000 CL days (8). A considerable rise was also seen when compared to previous historical cohorts, including pre-COVID-19 eras, as reported (8-10). We intended to replace central venous catheters with peripherally implanted central lines in our institution to reduce catheter infections.
Numerous studies highlight that a significant barrier to effective infection prevention measures is a lack of human and material resources. In addition to the effects of the COVID-19 pandemic, hand-washing soap, alcohol hand rubs, gloves, and other personal protective equipment have been identified as being in limited supply. Reusing sterile gowns because there were not enough of them during the pandemic’s first two waves may have played a significant role in the development of CLABSI (17). Catheter infections and related late-onset sepsis in neonates may be caused by a variety of causes, including the misuse or lack of equipment (18).
This study has some limitations. Firstly, the data was collected retrospectively from hospital data systems and medical records. Moreover, it lacked information on bundle compliance and other potentially influencing factors, including the nurse-to-patient ratio. One of the central line bundle’s tenets is its adherence to every bundle step; yet, since two principal elements were missing, we were unable to distinguish between the multiplicative effects of disregarding those two steps.
Based on our experience, close coordination between all parties, including the infection control committee, hospital administration, and health authorities, is required to prevent medical supply shortages and related issues. During the tender and purchase processes, healthcare authorities should highlight the end users’ prior experience, and they ought to communicate opinions in particular. Future studies should concentrate on better collaborating with the Ministry of Health throughout the procurement process, using artificial intelligence to determine precise numbers of medical devices used, and the financial implications of issues brought on by a lack of medical supplies.
In conclusion, even a three-month lack of NFC and SUF led to threefold CLABSI. The efficacy and ongoing success of CLABSI prevention depend on maintaining the materials’ continuity.