Introduction
Staphylococcus aureus, particularly methicillin-resistant Staphylococcus aureus (MRSA), is a major cause of serious hospital and community-acquired infections and is associated with increased health care costs, prolonged antibiotic treatment and hospitalization, morbidity, and mortality (1, 2). While glycopeptides (vancomycin and teicoplanin) have typically been used in the treatment of MRSA infections, considerable treatment failures have been reported in recent years, with tigecycline, daptomycin and linezolid being used for MRSA infections in which glycopeptide has failed for the past ten years (3-6). Some studies, however, have reported that MRSA isolates with reduced glycopeptide susceptibility were also less susceptible to daptomycin (7). The optimal antibiotic treatment choice for MRSA with reduced glycopeptide susceptibility remains a subject of debate.
Vancomycin susceptible MRSA isolates showed extensive heterogeneity in vitro with respect to vancomycin MICs and activity, which could affect treatment outcomes (8). Soriano et al. demonstrated that mortality was significantly higher when vancomycin was empirically used for the treatment of MRSA infections with high vancomycin MIC (>1 mg/L) (3). Similarly, a higher teicoplanin MIC value (>1.5 mg/L) was also reported as a risk factor in the unfavorable outcome and higher mortality rate among teicoplanin-treated MRSA bacteremia patients (5). Glycopeptide susceptibility breakpoints were lowered in recent guidelines due to the treatment failures of MRSA infections with higher MICs (9).
This study further explored the susceptibilities of MRSA isolates to vancomycin, teicoplanin, linezolid, daptomycin and tigecycline and the impact of glycopeptide minimum inhibitory concentrations (MICs) on clinical and microbiological outcomes.
Materials and Methods
Study Design and Identification of Patients
This retrospective cross-sectional study was conducted at a university hospital in TÜrkiye. We screened for adult patients with MRSA infections hospitalized between January 2013 and December 2017. Only the first episode of MRSA infection in each patient was included. Patients under 18 years old, with unavailable medical records or microbiological cultures, colonization with MRSA, and antistaphylococcal treatment ≤48 hours were excluded.
The demographic characteristics of the patients were obtained from the medical records. We collected the data of age, sex, pre-existing comorbidities, Charlson comorbidity index, American Society of Anesthesiology (ASA) score, receipt of prior antimicrobial therapy for >48 hours, and history of surgical and MRSA infections for all patients. MRSA infections were classified according to the definitions of the Centers for Disease Control and Prevention (CDC) (10). The origin of the infection (community-acquired, healthcare-associated infections-community onset, healthcare-associated infections-hospital onset), presence of septic inflammatory response syndrome (SIRS), sepsis and septic shock (sepsis criteria valid at the time of study were used), need for mechanical ventilation, central venous catheter, prosthetic material were all recorded.
All patients with MRSA bacteremia were evaluated routinely with transthoracic echocardiography (TTE) for infective endocarditis. Transesophageal echocardiography (TEE) was performed when TTE imaging was non-diagnostic or clinical suspicion of infective endocarditis was high. In some clinical scenarios, other imaging techniques (cardiac computerized tomography, magnetic resonance imaging and nuclear imaging) were also considered. Infective endocarditis was rejected in patients who did not meet definitive or possible modified Duke criteria, or an alternative diagnosis was confirmed.
In this study, a loading dose of teicoplanin 6 mg/kg for three doses, followed by a maintenance dose of 6 mg/kg q24h and vancomycin 500 mg q6h dose, were used in patients with normal renal function. Antibiotic dose adjustments were done in patients with renal impairment according to creatinine clearance. Prior glycopeptide therapy was defined as the use of vancomycin or teicoplanin for >48 h in three months before the occurrence of MRSA infection.
Treatment failure was described as culture positivity for >7 days, antibiotic switching because of clinical unresponsiveness, or mortality. We used 1 mg/L MIC value for treatment failure, which has been reported as a treatment failure cut-off in previous reports (3, 4). To reflect these concerns, patients with MRSA infections were divided into the following two groups: low-glycopeptide MIC group (glycopeptide MIC of ≤1 mg/L) and high-glycopeptide MIC group (glycopeptide MIC of >1 mg/L).
Isolates and Microbiological Methods
Various clinically important MRSA isolates recovered from hospitalized patients were used in this study. Only the first isolate for each patient was used for laboratory investigations. Isolates were stored in tryptic soy broth with 15% glycerol at -20°C until the time for in vitro testing. The quality control of susceptibility testing was performed using the ATCC 29213 reference strain. Antimicrobial susceptibility tests were carried out on Mueller-Hinton agar using Liofilchem® MIC Test Strips (Liofilchem Inc., Italy) for gradient testing. Vancomycin, teicoplanin, linezolid, daptomycin and tigecycline MICs were evaluated under blinded conditions without knowing any clinical outcome in accordance with the European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations. The effect of MIC values on clinical outcomes was evaluated. All procedures were performed in the same laboratory by a single observer within four weeks.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 15.0 (IBM Corp., Armonk, NY, USA). The descriptive statistics are shown as mean (±standard deviation) for normally distributed variables, median (min-max) for not normally distributed variables, and frequency and percentage (%) for nominal variables. The significance of the difference between the groups in terms of means and median values was compared using t-test and Mann-Whitney test, depending on whether the data was normally distributed or not. The nominal variables were analyzed using the Pearson Chi-square or Fisher exact test. The parameters affecting the group variables were evaluated with univariate analysis, after which the parameters with p<0.20 were included in the multivariate logistic regression analysis. Independent risk factors and risk coefficients were determined. Two-tailed Spearman’s rho was used to calculate the correlation coefficients between vancomycin, teicoplanin, daptomycin, tigecycline and linezolid MIC values of MRSA isolates. A p-value <0.05 was considered statistically significant.
Results
Microbiological Assessment
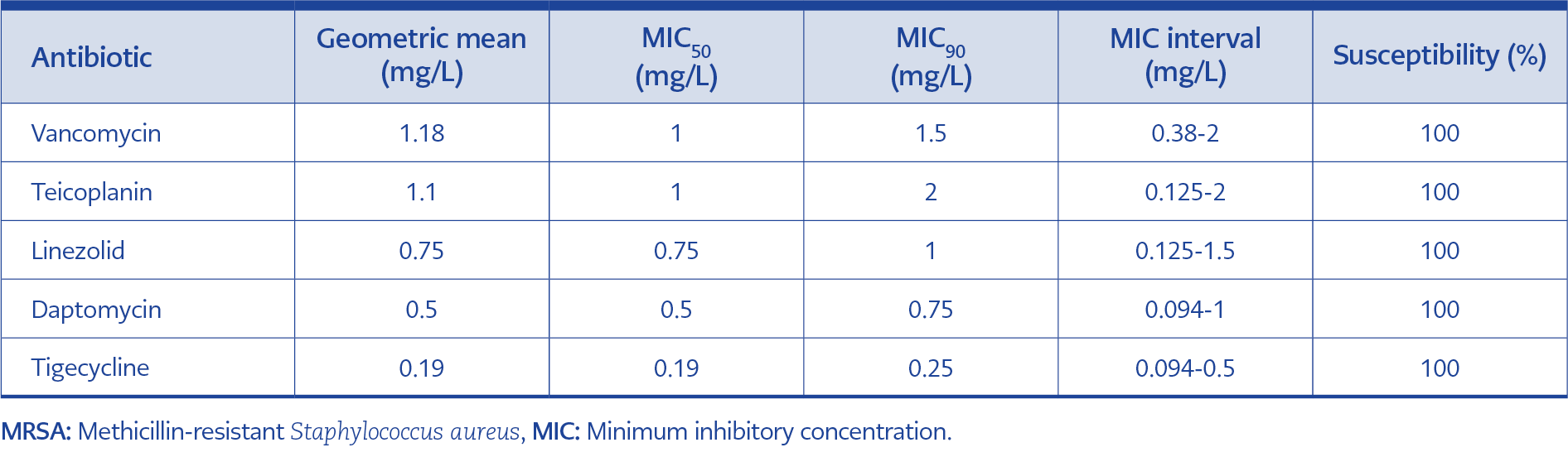
Table 1. Vancomycin, teicoplanin, linezolid, daptomycin and tigecycline susceptibilities of clinical MRSA isolates (n=104).
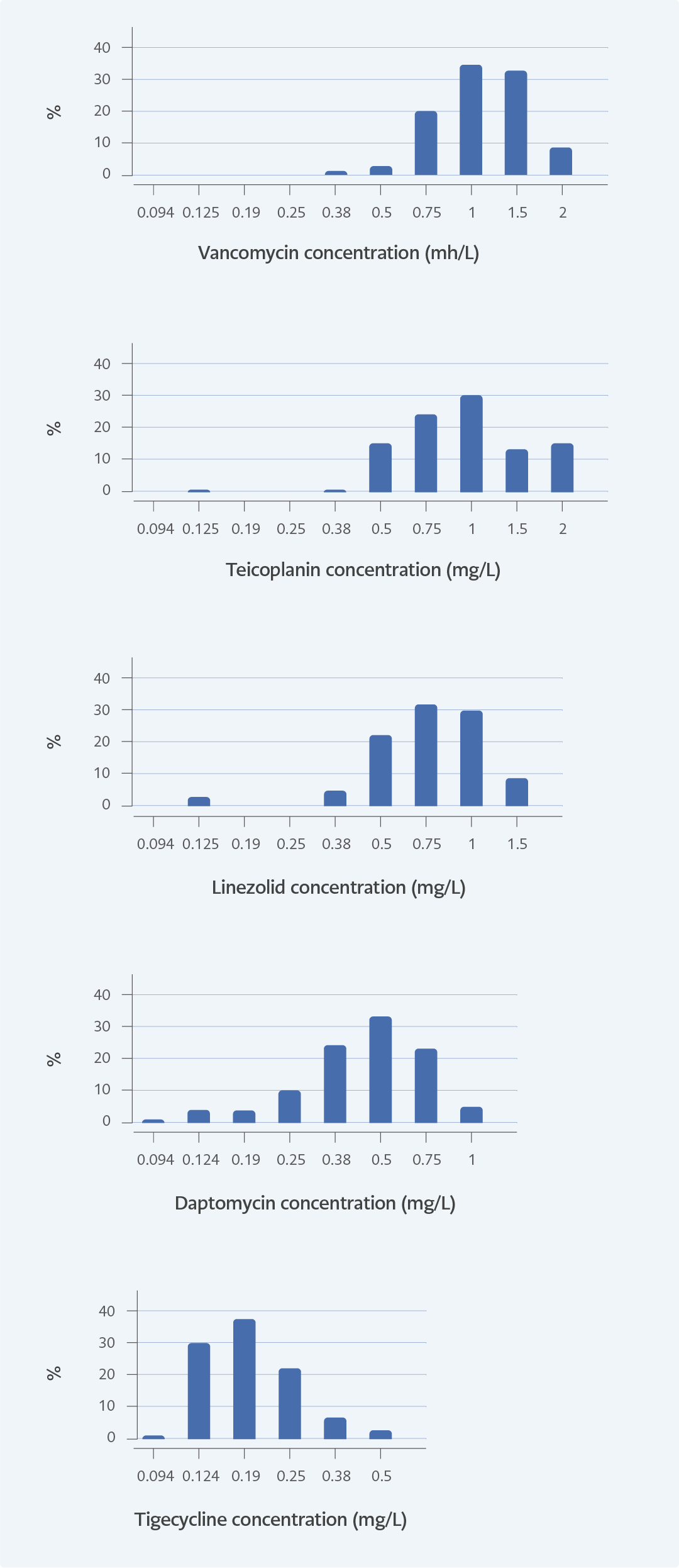
Figure 1. TMICs distributions for vancomycin, teicoplanin, linezolid, daptomycin and tigecycline of MRSA isolates (n=104).
A total of 159 MRSA isolates from various clinical samples were identified, and a total of 104 patients infected with MRSA strains were included in the study. The MIC90 values for vancomycin, teicoplanin, linezolid, daptomycin and tigecycline were 1.5 mg/L, 2 mg/L, 1 mg/L, 0.75 mg/L, and 0.25 mg/L, respectively (Table 1). All isolates were susceptible to the tested antibiotics according to EUCAST standards. Vancomycin and teicoplanin MICs higher than 1 mg/L were documented in 30 (28.8%) and
43 (41.4%) of all isolates, respectively. The number of isolates with a MIC of 2 mg/L was nine (8.7%) for vancomycin and 16 (15.4%) for teicoplanin. Figure 1 demonstrates the MIC distributions of the antibiotics tested for MRSA isolates.
The MIC correlations between vancomycin, teicoplanin, linezolid, daptomycin and tigecycline were evaluated, and a significant correlation was identified between the MIC values for teicoplanin and daptomycin (r=0.278, p=0.002). The MIC value of vancomycin was significantly correlated with linezolid (r=0.211, p=0.020) and daptomycin MICs (r=0.184, p=0.044). A positive correlation was detected between teicoplanin and vancomycin MICs (r=0.329, p=0.000) (Table 2).
Clinical Characteristics
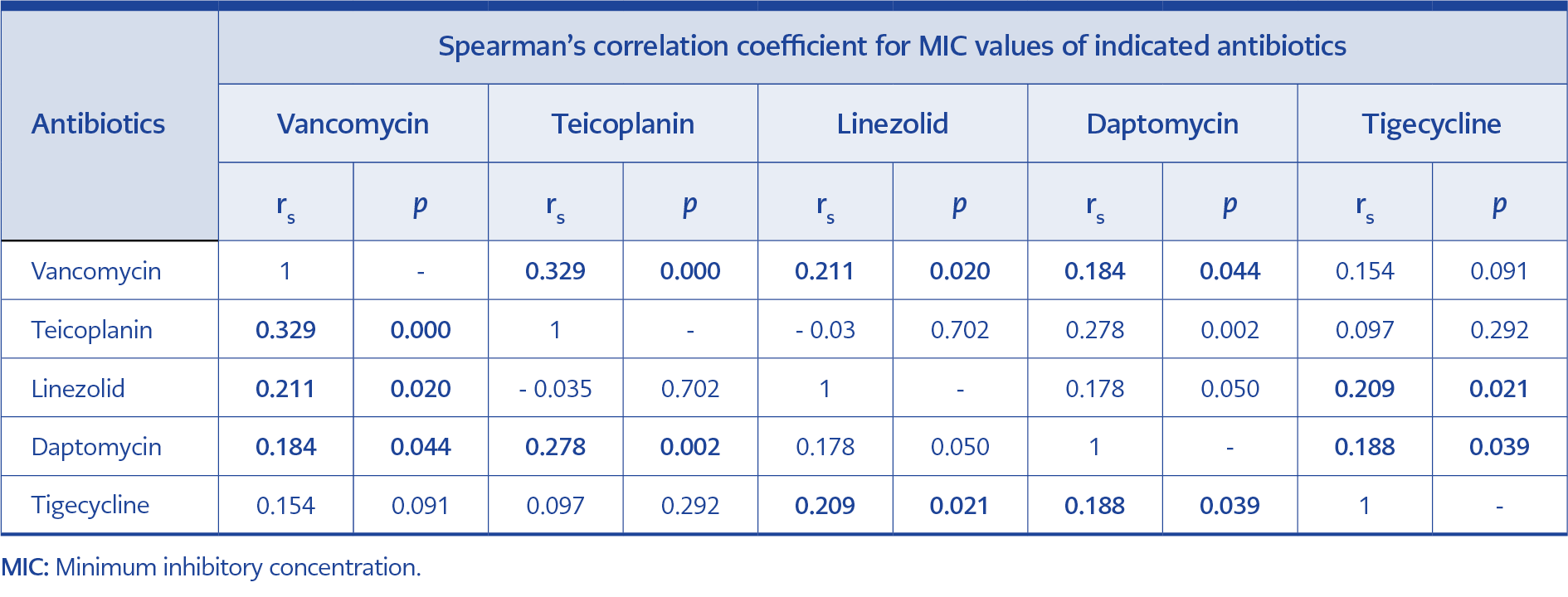
Table 2. Correlations between MIC values of antibiotics tested (n=104).
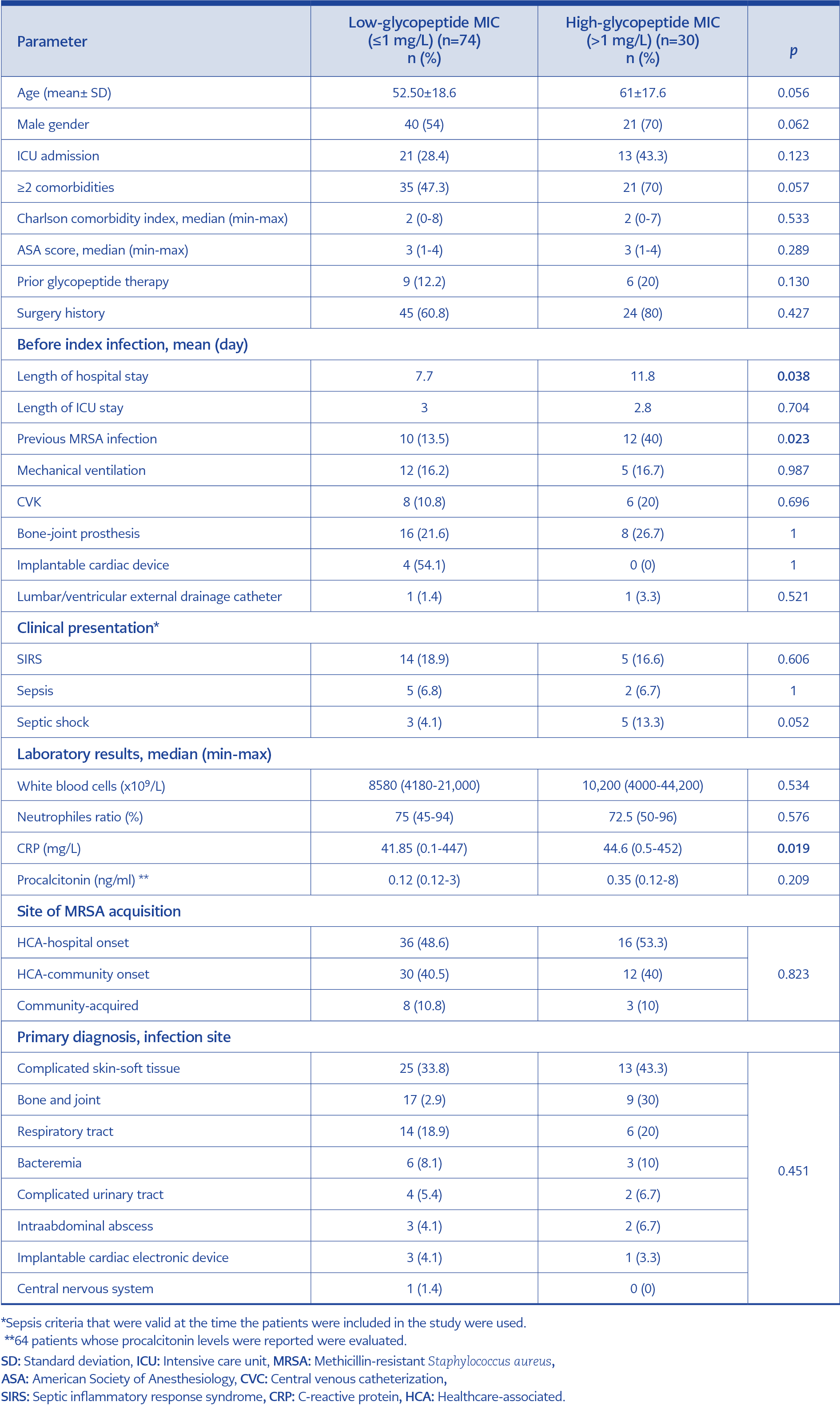
Table 3. Baseline characteristics, demographic, clinical and laboratory findings of patients (n=104).
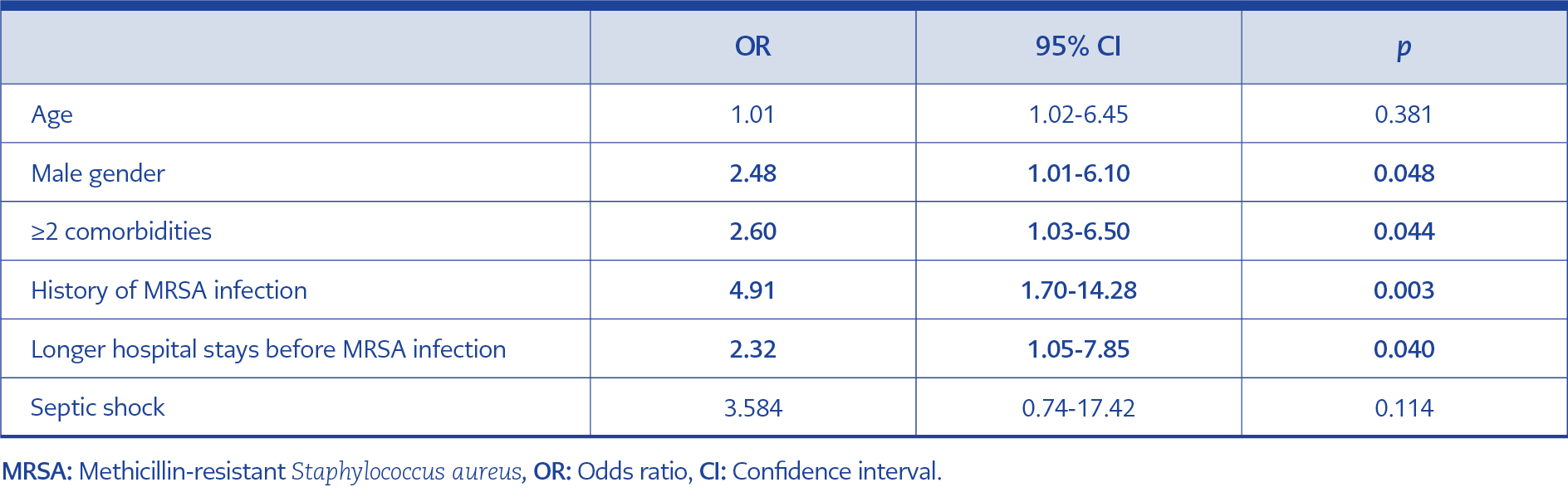
Table 4. Risk factors associated with high-glycopeptide MIC values identified using multivariate logistic regression analysis (n=104).
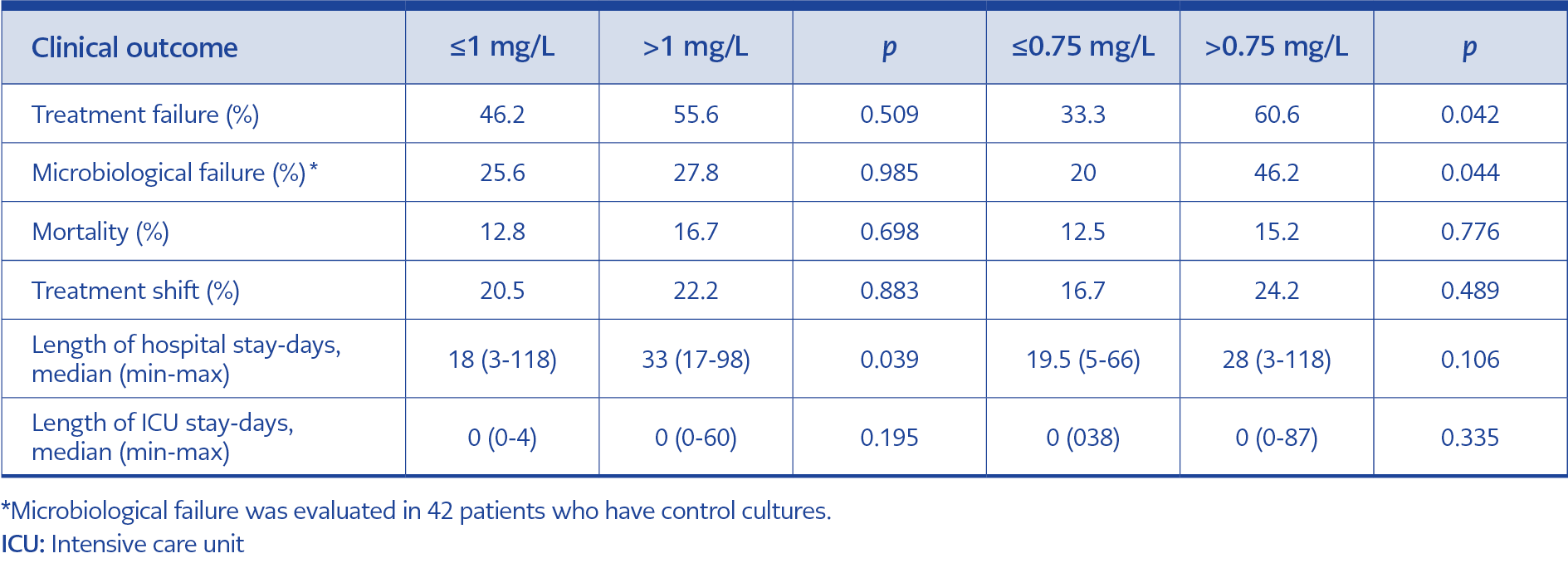
Table 5. The effects of teicoplanin MIC values on clinical outcome in MRSA infections treated with teicoplanin (n=57).
The final cohort included 104 patients with MRSA infections according to the inclusion criteria, of which 74 (71.2%) patients were classified as MRSA infections in the low-MIC group (≤1 mg/L), and the other 30 (28.8%) patients in the high-MIC group (>1 mg/L). The majority of the isolates were obtained from complicated skin-soft tissue (49.9%) and respiratory tract infections (17.2%). MRSA bacteremia was detected in nine patients (8.6%). Table 3 presents the baseline characteristics, demographics, and clinical and laboratory findings of the patients. Being of the male sex (odds ratio [OR]=2.48, 95% confidence interval [CI]=1.01-6.10, p=0.048), having ≥2 comorbidities (OR=2.48, 95% CI=1.03-6.50, p=0.044), history of MRSA infection (OR=4.91, 95% CI=1.70-14.28, p=0.003) and a longer hospital stay prior to MRSA infection (OR=2.32, 95% CI=1.05-7.85, p=0.040) were identified as significant risk factors associated with high-glycopeptide MIC values identified using multivariate logistic regression analysis (Table 4).
The most frequently prescribed antistaphylococcal agent was teicoplanin 57 (54.9%) followed by linezolid 17 (16.3%). Vancomycin was only used in four (3.8%) patients. The overall treatment failure was recorded as 36.5%, which rose to 49.2% in patients treated with glycopeptide antibiotics (vancomycin or teicoplanin).
A subgroup of 57 patients were analyzed that were infected with MRSA and treated with teicoplanin. Since the number of patients treated with vancomycin was small, these four patients were not included in this analysis. Treatment failure was recorded in 28 (49.1%) patients treated with teicoplanin. In MRSA isolates with a teicoplanin MIC of >0.75 mg/L, the microbiological failure and treatment failure when treated with teicoplanin was 46.2% (p=0.044) and 60.6% (p=0.042), respectively (Table 5). However, a teicoplanin MIC of >0.75 mg/L was not associated with mortality or length of hospital and intensive care unit (ICU) stays. In the study population, a teicoplanin MIC of >1 mg/L was associated only with a longer hospital stay (p=0.039).
Discussion
There are a number of possible reasons for treatment failure in MRSA infections, including inadequate surgical debridement, poor source control, and antibiotic pharmacodynamic factors (11). The antimicrobial resistance pattern of MRSA isolates requires close monitoring, particularly for antibiotics that are commonly used for treatment (12). The frequent use of glycopeptides as the drug of choice for treatment has putatively led to the selection of these isolates with reduced susceptibility to glycopeptides (13). There are a growing number of studies reporting the discordance between glycopeptide susceptibility and clinical success in MRSA infections. In this study, all MRSA isolates were susceptible to vancomycin, teicoplanin, linezolid, daptomycin and tigecycline according to EUCAST standards. Still, the overall treatment failure was recorded as 36.5%, and this rate rose to 49.2% in patients treated with a glycopeptide antibiotic.
This study showed a significant positive correlation between the MICs for glycopeptides and daptomycin, as well as vancomycin and linezolid. Similarly, Hsieh et al. reported a positive correlation between glycopeptides and daptomycin MICs (14). It is plausible that the mechanisms of reduced glycopeptide susceptibility in MRSA, including a thickened cell wall, changes in cellular metabolism and enhanced cell wall turnover, may affect the antimicrobial action of daptomycin (15). These MIC correlations may need to be considered when choosing another agent in cases with glycopeptide treatment failure.
Male sex, two or more comorbidities, history of MRSA infection and longer hospital stays were independent predictors of high glycopeptide MICs in the logistic regression analysis. Lubin et al. also reported that a history of MRSA bacteremia was a risk factor for high vancomycin MIC (16). On the other hand, prior vancomycin exposure was reported as an important risk factor for high glycopeptide MICs in several studies (16-18). In our cohort, 12.2% of patients infected with low-glycopeptide MIC MRSA had prior glycopeptide antibiotic exposure, and the rate increased to 20% in patients with high-glycopeptide MIC; it was not statistically significant (p=0.130). This result may be due to the limited number of patients included in the study and the use of non-glycopeptide antibiotics in prior MRSA infections.
Epidemiological studies showed that men had an increased risk for several infections, although the underlying biological mechanism was not fully understood (19). Some studies have also shown that S. aureus nasal carriages and infections were at a higher rate in male gender (20, 21). The invasive MRSA infection incidence rate ratio of men compared to women was reported as 1.8 by Brandl et al. (22). Our study also showed that male gender was an independent risk factor for higher glycopeptide MIC in MRSA infections. This association could be related to a higher incidence of MRSA nasal carriage or disease severity in the male gender, as reported in the literature.
EUCAST recommended broth microdilution (BMD) for glycopeptide MIC assessment (9). BMD is a labor-intensive technique that may not be used routinely in many laboratories. Gradient strip methods may be used as an alternative for glycopeptide MIC testing. The systematic review and meta-analysis study conducted by Diaz et al. also supported this view. They showed that there were no significant differences between the results of the pooled means of vancomycin MICs for all MRSA isolates reported with BMD and gradient methods (23). In this study, we used gradient strip methods to assess glycopeptide MIC.
Vancomycin and teicoplanin MICs higher than 1 mg/L were documented in 30 (28.8%) and 43 (41.4%) of all isolates, respectively. Although vancomycin and teicoplanin are the current mainstay for MRSA treatment, there have been a number of published reports of reduced clinical efficacy associated with vancomycin MICs between 1 mg/L and 2 mg/L (3, 4, 24). The vancomycin MIC value for treatment failure and mortality in MRSA infections has been commonly reported as 1 mg/L in literature (3, 4, 25). The Infectious Disease Society of America (IDSA) Guideline recommended considering the use of an alternative agent for MRSA infections with vancomycin MIC ≥ 1.5 mg/L in critically ill patients (26). Although teicoplanin is not approved for use in the USA, it is widely used in Türkiye and Europe. While several studies have focused on the impact of vancomycin MICs on clinical outcomes of MRSA infections, few studies have evaluated the effects of teicoplanin MICs on the outcomes of MRSA infections (5, 27, 28). In a study by Chen et al., teicoplanin MIC of <2 mg/L was associated with a lower treatment failure (12.9% vs 36.7%, p=0.02) in patients with MRSA pneumonia (28). Chang et al. reported that a teicoplanin MIC value >1.5 mg/L might be associated with unfavorable outcomes and higher mortality in MRSA bacteremia (5). Our study results showed that a teicoplanin MIC of 0.75 mg/L was a more precise cut-off for both treatment and microbiological failures. Although the majority of the patients were treated with teicoplanin this study showed a positive correlation between vancomycin and teicoplanin MICs. For this reason, a 0.75 mg/L cut-off may be precise for both glycopeptides. Clinicians should closely follow clinical and microbiological data when using glycopeptides to treat MRSA infections with glycopeptide MIC >0.75 mg/L. In a meta-analysis, there were no statistically significant differences in the risk of death between patients infected with S. aureus exhibiting high and low vancomycin MICs (29). Similarly, teicoplanin MIC >0.75 mg/L was not associated with mortality in our cohort.
There were several limitations in this study. First, as this was a single-center, retrospective study, the number of cases was small, which meant the number of patients with MRSA bacteremia was limited. However, most patients had complicated skin-soft tissue infections and pneumonia, which carried the risk of bacteremia. Second, we did not perform molecular analysis for an epidemiological survey to identify the specific MRSA strains with specific resistant genes which could influence MIC values. The number of patients using vancomycin was very low in this study, so the recommended threshold MIC level and treatment failures may not be attributed directly to vancomycin, although we showed a positive correlation between vancomycin and teicoplanin MIC. Since teicoplanin was the most frequently used glycopeptide in our hospital, and so in this study, these results could be interpreted as being more related to teicoplanin. Finally, we did not determine the ratio of heterogenous vancomycin-intermediate S. aureus (hVISA) in our isolates which could have an impact on treatment failure.
While the study population was small in size, the critical MIC value, which suggested treatment failure as well as microbiological failure in the teicoplanin-treated MRSA infections, was >0.75 mg/L rather than >1 mg/L in this study. The identification of high-risk patients for treatment failure by considering the glycopeptide MIC values is crucial, especially in patients with severe MRSA infections.