Introduction
Cystic echinococcosis (CE), caused mainly by Echinococcus granulosus, is a parasitic disease common in Mediterranean countries such as Türkiye (1). Although it can occur anywhere in the body, it predominantly affects the liver (2). The disease is often asymptomatic; thus, cysts are often detected incidentally during imaging studies performed for other purposes. Symptoms like right upper quadrant pain, abdominal fullness, jaundice, and compression occur depending on the size of the cyst and its relation with adjacent structures (3, 4). CE is classified into five types according to the Gharbi classification based on cystic density, membrane detachment, solid, and calcified areas. Cysts, according to Gharbi, are as follows: type I pure cystic; type II cyst with membrane separation; type III cyst containing multiple septa and daughter vesicles; type IV high internal echo, hyperechoic heterogeneous solid mass appearance; type V calcified thick-walled cyst. While types I-III are considered fertile, type IV is rarely fertile, and type V is inactive. The World Health Organization (WHO) classification, also depending on cyst morphology, consists of types ranging from CE1 to CE5 (5). Our Radiology Department prefers the Gharbi classification, so we used the Gharbi classification in our study.
Among potential complications related to the treatment of CE are intra-abdominal dissemination, biliary fistulization, and anaphylactic reactions. Medical intervention, administered pre- and post-operatively, is frequently used to complement surgical or percutaneous procedures. Mebendazole and albendazole are benzimidazole derivates used in the medical treatment of CE. They inhibit adenosine triphosphate (ATP) synthesis by obstructing glucose utilization. Although conventional surgical approaches remain the primary treatment modality for CE, percutaneous techniques have been developed specifically for cases with high surgical risk and complex cystic attributes. Catheter-based interventions, including the PAIR (puncture, aspiration, injection, re-aspiration) procedure and modified catheter treatments, are appropriate treatment options for selected cases at anatomically suitable locations (6).
While comparable investigations have been undertaken across various regions of Türkiye, to the best of our knowledge, there is no analogous study specific to our department or province in the accessible literature. We conducted a retrospective analysis of cases with intra-abdominal cystic echinococcosis presented at our General Surgery Department in Çanakkale province, focusing on variables such as age, gender, presenting symptoms, cyst localization, Gharbi classification, and the modality of surgical intervention or medical treatment.
Materials and Methods
This study was designed as a retrospective cohort study. Cases who were admitted to our General Surgery Department with the diagnosis of intra-abdominal cystic echinococcosis between January 1, 2012, and January 1, 2022, were examined. In this study, evaluation was conducted on various parameters of the cohort, including age, residential locality, gender, presenting symptoms, duration of symptoms, cyst localization within the organ system, Gharbi classification, surgical treatments (such as laparoscopy), medical treatments (e.g., albendazole or mebendazole), and treatment outcomes (such as remission or recurrence).
Patients 18 years of age or older and who were eligible to give written consent were included. Data from minors, cases with extra-abdominal involvement, pregnant, or who were not eligible for written consent were excluded from the study.
Data was acquired via the Patient Information Management System. Prescription records, discharge summaries, and laboratory test results were evaluated within the automated system, with subsequent data transferred to case forms. Identity information was intentionally excluded from these forms.
The Çanakkale Onsekiz Mart University Ethics Committee approved the study on March 22, 2022 with the decision number 2022-05.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 23.0 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequency (n) and percentage (%). Descriptive statistics for normally distributed variables were presented as mean values with standard deviation, while non-normally distributed variables were presented as median values. The Shapiro-Wilk test was performed to assess the normal distribution of the data. Additionally, data visualization was facilitated via the creation of tables and graphics in Microsoft Excel, enhancing the depth and clarity of the result presentation.
Results
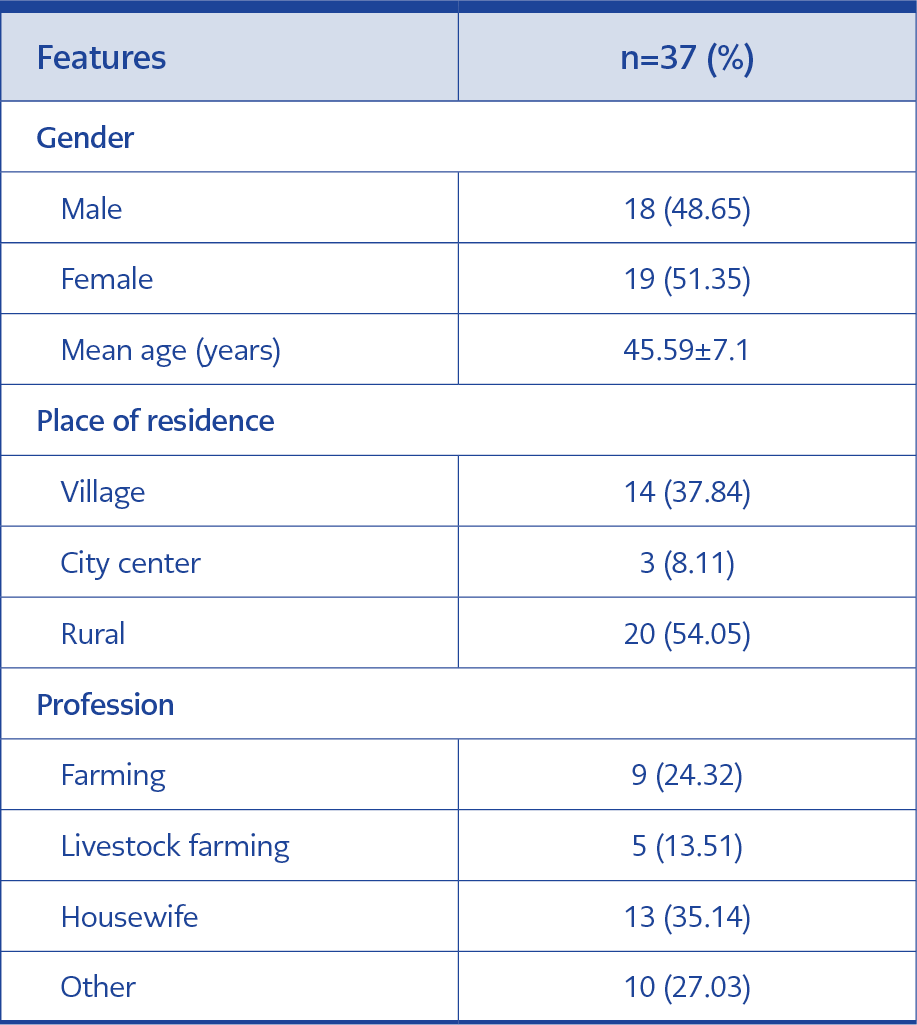
Table 1. Demographic characteristics of cystic echinococcosis cases.
The study cohort consisted of 37 cases; the mean age was 45.59±7.1 years, and 19 (51.35%) were female. The majority of cases resided in urban districts (n=20 [54.05%]), and only 14 (37.84%) were engaged in animal husbandry or agriculture. Table 1 summarizes the demographic data of the cases included in the study.
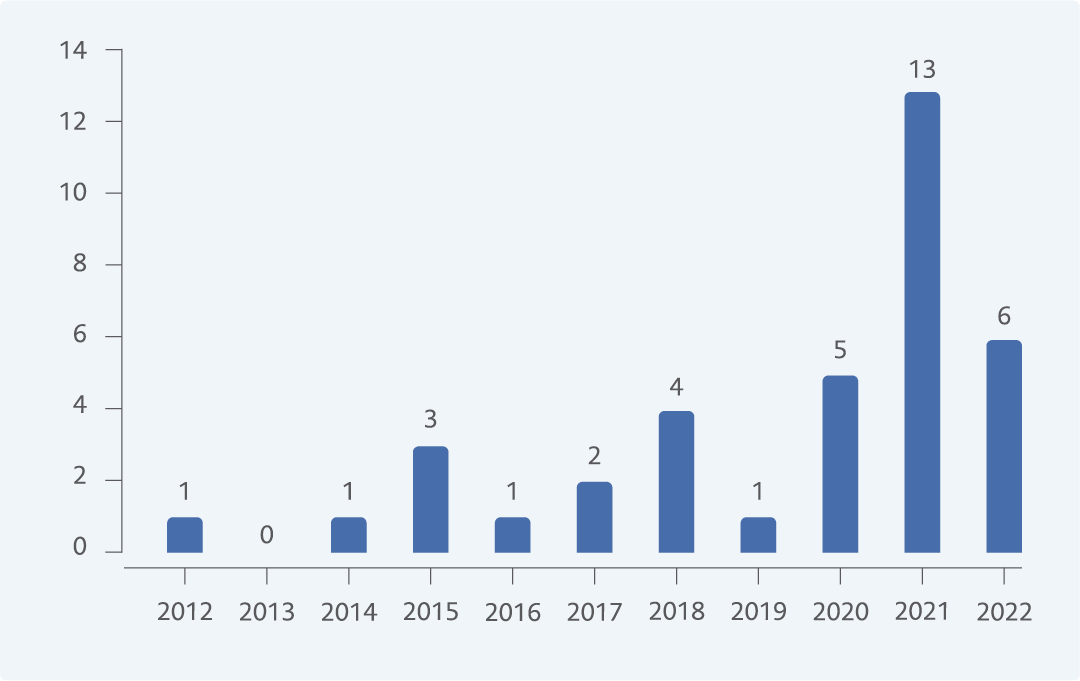
Figure 1. Number of cases by years.
When the population of each year in our province was correlated with our cohort, the incidence varied between 0-0.000021 cases per year. The most common complaints were abdominal pain 67.57% (25/37), malaise 5.41% (2/37), and pruritus 2.70% (1/37). However, 24.32% (9/37) of the cases had no complaints. The mean symptom duration was 4.3±1.02 months. The majority of the cases (35.14%) were diagnosed in 2021 (Figure 1).
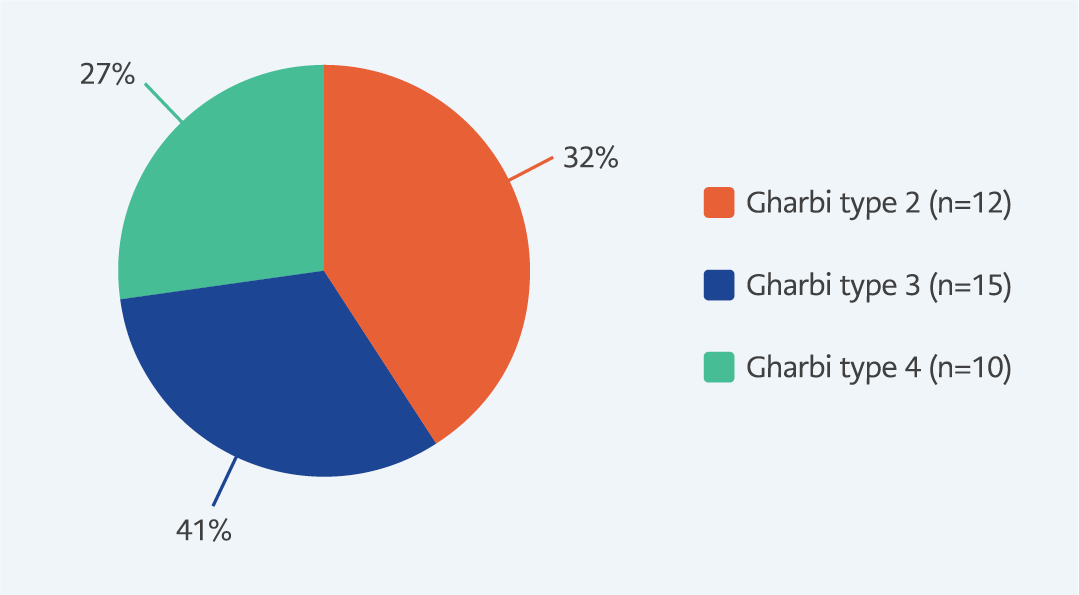
Figure 2. Gharbi type of cases.
Cystic echinococcosis diagnosis was confirmed by visualization of the cuticular membrane by means of pathological examination in all cases. All diagnoses were established through radiological means, with abdominal computed tomography (CT) utilized in 27 cases, abdominal ultrasonography (USG) in eight, and abdominal magnetic resonance imaging (MRI) in two. Positive results from E. granulosus immunoglobulin G (IgG) antibody (IHA) testing were obtained in 29 cases. Isolated liver involvement was observed in 34 cases, while isolated spleen involvement occurred in 3 (8.11%). The mean cyst diameter measured 106.32 mm (range 50-200), including 29 cases with solitary cysts, six with double cysts, and one with triple and the other with quadruple cysts. Most of them (n=15) were Gharbi type III (Figure 2).
According to our investigation, all cases were given albendazole as medical treatment. Cystotomy with capitonage was performed in 30 cases, while laparoscopic pericystectomy was performed in seven. The mean duration of hospitalization was 8.29 days. Three cases underwent hypertonic saline lavage; in two, 0.04% chlorhexidine gluconate solution was used, and in the remaining 32, 50% diluted povidone-iodine solution was used. Intraoperative rupture occurred in one case. Notably, 36 (97.30%) cases exhibited complete resolution, whereas 1 (2.70%) case experienced recurrence. Early and late complications were observed in 12 (32.43%) cases, biliary fistula in 5 (13.51%), and secondary bacterial infections in 4 (10.81%). In the cohort studied, a total of 3 (8.11%) cases exhibited splenic involvement; all underwent laparoscopic pericystectomy accompanied by hypertonic saline lavage. Only one case resulted in a secondary bacterial infection. There were no documented instances of recurrence among cases with splenic involvement.
Discussion
We retrospectively analyzed cases of intra-abdominal cystic echinococcosis in Çanakkale province, whose follow-up and treatment were concluded within our general surgery clinic. Although the incidence of CE in some provinces of Türkiye is known, it has not been studied throughout the country. Concerning Çanakkale province, we were able to identify only a few case reports in the literature without any epidemiologic background information (7, 8). We also were not able to identify any study concerning the incidence or prevalence in our province in TUrkish or English literature.
The incidence of cases is estimated at 1.59 (in one hundred-thousandth) or lower for most of Türkiye, including our province (9). Incidence of intra-abdominal CE cases in our department varies from 0 to 2.1 (in one hundred-thousandth). This range is only at the peak higher than the estimated incidence. It is important to note that our operations correlated to the relative year do not represent the incidence of cystic echinococcosis, as they only reflect surgically treated, solely intra-abdominal cases managed in our department. Even so, these incidents are the only reference value available to us for now. Additional data could provide a better and more reliable understanding of CE in our region.
Although our study did not include pregnant cases diagnosed with CE, symptomatology, like abdominal pain, showed similarities to our cohort, as presented by the study conducted by Şahin et al. (10). Thus, this is a good reminder that physicians should always be aware of environmental, and labor-related risk factors. In the study cohort of Türkoğlu et al., 58.4% of 238 CE cases were female, and the mean age was 40.6 years. The mean age in our study was 45.59 years (11). In a similar study evaluating the characteristics of adult cases with CE in the Eastern Anatolia region, 59.1% of the 66 cases were female (12). A predominance of female cases of 51.35% was observed in our cohort, while the female/city population ratio was 49.62% during the study period. Also, for the same period, the female-to-population ratio in Türkiye was 49.85% (13), supporting that the incidence of E. granulosus is higher in women, although the male population is higher. The increasing prevalence prompts consideration of multifaceted factors. Among plausible explanations are hormonal influences, increased exposure of women to potential risk factors such as livestock or agricultural settings, as well as increased accessibility to healthcare services facilitating more frequent diagnosis among women. Such findings may also reflect inherent demographic variances and methodological disparities across studies. Nevertheless, further studies and meticulous data analysis are imperative to elucidate the precise underpinnings of these associations.
Concerning the demographic and clinical attributes of E. granulosus infection, our results are different from those of TÜrkoğlu et al. (11). Our analysis indicated that most cases were concentrated within urban districts, and only a minority involved in animal husbandry or agricultural activities. Conversely, Türkoğlu et al.’s research, with a larger cohort compared to ours, revealed a substantial proportion of patients residing in rural areas (11). In both studies, abdominal pain emerged as the predominant complaint, exhibiting a prevalence of 67.57% in our study and 65.6% in TÜrkoğlu et al.’s study. Furthermore, TÜrkoğlu et al.’s study, which encompassed not only general surgery but multiple clinics, identified additional symptoms among patients, including cough (23.3%, n=42), chest pain (19.4%, n=35), nausea and vomiting (14.4%, n=26), dyspepsia (11.1%, n=20), fever (7.8%, n=14), shortness of breath (7.8%, n=14), hemoptysis (6.7%, n=12), jaundice (3.9%, n=7), hydatoptysis (3.9%, n=7), bone discharge (0.8%, n=2), back and lower back pain (0.4%, n = 1), dysuria (0.4%, n=1), and syncope (0.4%, n=1) (11). In our study, weakness was reported by 5.41% (2/37), while itching was noted by 2.70% (1/37). Conversely, 24.32% of patients (9/37) remained asymptomatic. As our study was confined to the General Surgery Department, the discrepancy among symptoms indicates the importance of the relation between symptoms and organ/system involvement.
The management of hydatid disease consists of a range of therapeutic modalities, including systemic medical treatment, surgical interventions, and percutaneous drainage. Predominantly, surgical intervention is prioritized; medical-only treatment, particularly employing drugs such as albendazole, is reserved for cases deemed uncomplicated, patients presenting with multiple cysts, individuals not amenable to surgical intervention, or those refusing surgical options (14). Surgical treatment modalities evolved from internal capsule excision to various capsule excision modalities and interventions, including laparoscopy and extending even to liver transplantation (15). We found that surgical interventions such as laparoscopic pericystectomy provided high cure and low recurrence rates. According to the TUrkish HPB Surgery Association Consensus Report on hepatic cystic echinococcosis (HCE), surgical treatment is indicated in large uncomplicated CE2 and CE3b cysts with many daughter cysts (16). Gharbi type IV cysts are mostly considered inactive, and in uncomplicated type IV cysts, a watch-and-wait strategy is advised (17); surgery is still performed on patient-based decisions (6, 18, 19).
On the other hand, in a study encompassing multiple treatment modalities with a cohort of 491 patients, it was concluded that one of the most important causes of complications and, therefore, mortality in CE patients was treatment strategies, including watch-and-wait as a main factor for mortality (6). While 32.43% of our patients encountered various complications, biliary fistula and secondary bacterial infections were the most prominent ones, and we had no mortality. PAIR combined with albendazole has been shown to be an effective treatment modality in patients with uncomplicated cysts (20). According to the results of a recently published meta-analysis, treatment outcomes exhibit enhancement when surgery or PAIR is combined with benzimidazole (21). Although PAIR has favorable results in selected patients, we could not include this treatment modality because it was not performed at our institution during the study period. The main agent to be considered for the medical treatment of CE was found to be albendazole (10, 21). In our study, all surgical interventions were combined with perioperative albendazole management.
The average recurrence time for liver manifestation was reported as 16.5 months by Yosra et al. (22). In a multicenter study, conducting high-volume training and education hospitals in major cities, the recurrence rate was more than 27% (19). Our recurrence rate of 2.7% was remarkably low. This difference might be, at least to a level, attributed to our high Gharbi type IV patients or a difference in follow-up protocols. No recurrence occurred in our patients with splenic manifestation; the only recurrence was in a patient with liver manifestation after 27 months. Whom 50% diluted povidone iodine solution was used as a scolicidal agent, and albendazole was given in the perioperative period.
Our study has several limitations. First, it has a small sample size covering only intra-abdominal CE patients. Second, we could not perform PAIR, although it has been shown to be an effective treatment modality in patients with uncomplicated cysts. Third, our study did not cover subtypes of E. granulosus because of retrospective design. Investigating the genetic diversity of E. granulosus strains in our region could have provided valuable information about the epidemiology and transmission dynamics of hydatid disease. Echinococcus spp. has been revealed to have ten genetic strains, including E. granulosus sensu stricto G1 to G3, which is the most widely spread type (23). A study conducted in Van/Turkey revealed that all samples were E. granulosus sensu stricto G1, with 9.5% having single nucleotide polymorphism (24). In addition, A recent study has been conducted to develop molecularly targeted drugs aimed at specific subtypes (25). As molecular therapy options are emerging, planning a prospective study covering regional subtypes may be beneficial for future treatment options.
Our retrospective review of cystic echinococcosis cases in a single tertiary care university hospital revealed that the disease predominantly affected individuals from urban districts, and the most common complaint was abdominal pain. Occupation in agriculture or animal husbandry does not seem to be the main risk factor in our region. Radiologic imaging, especially abdominal CT, ultrasound, and MRI, played an important role in the diagnosis. The diagnosis was confirmed by visualization of the cuticular membrane by means of pathological examination in all cases. Surgical intervention, especially cystotomy with capitonage and laparoscopic pericystectomy, resulted in high cure rates and low recurrence rates.