Introduction
Hepatitis C virus (HCV) is an enveloped, single-stranded, positive polarity RNA virus from the Flaviviridae family. It is part of the Hepacivirus genus, wrapped in a lipid bilayer containing two viral glycoproteins (E1 and E2) (1). HCV infection is a major public health problem that can lead to complications such as cirrhosis and liver cancer (2). Approximately 85% of people with acute HCV infection progress to chronic HCV infection. The World Health Organisation (WHO) estimates that about 58 million people worldwide are affected by chronic HCV infection, with about 1.5 million new infections each year and about 290,000 deaths (2).
The distribution of HCV genotypes (GTs) in a geographical area can be altered with an increase in cultural diversity (3). Türkiye’s historical importance as a crossroads between East and West, coupled with its role as a major transit and migration route, has contributed to a diverse population in the region.
Because of the high mutational potential of HCV, the phenotype can change in a short time, leading to escape from host defense, cell tropism, changes in virulence, and resistance to antiviral agents. These immune escape mutations can lead to chronic infections (4). Although treatment without determining HCV GTs and subtypes is possible with pan-genotypic HCV drug regimens, it is important to determine the GT and subtype in centers using genotype-specific regimens (5, 6). The most common GT worldwide is GT1. The current diagnostic methods for HCV infection and the determination of the required treatment duration are based on the detection of total anti-HCV antibodies, HCV core antigen, HCV RNA levels, and HCV genotyping (7-9).
The Centers for Disease Control and Prevention (CDC) has estimated that approximately 21% of individuals living with HIV in the United States are also infected with HCV (10). Given that both HIV and HCV can be transmitted via blood, a significant risk factor for both HIV and HCV infection is injection drug use. The sharing of needles or other drug injection equipment increases the risk of contact with HIV or HCV-infected blood. The prevalence of co-infection varies considerably according to the risk group in question. For instance, the prevalence of co-infection among men having sex with men (MSM), high-risk heterosexuals, and individuals who use injection drug equipment is notably higher than in other risk groups (10).
Among persons living with HIV in the United States, an estimated 6 to 30% have HCV co-infection. However, these rates vary based on the composition of risk factors for acquiring HIV in any given cohort. In particular, higher HCV prevalence is observed among cohorts of persons with HIV who inject drugs. It has been observed that the onset of cirrhosis occurs earlier in people with HCV and HIV co-infection than in those with HCV mono-infection (11-14).
We hypothesized that due to the geographical and geopolitical location of Türkiye, the epidemiology of HCV infection in the region might change as a result of increased immigration. This study aimed to contribute to the epidemiological data by examining HCV seroprevalence, viremia rates, HCV/HIV co-infection rates, and genotypes in patients admitted to Sincan Training and Research Hospital in Ankara province, having increased immigration in the last three years.
Materials and Methods
This is a retrospective cross-sectional study. We collected the patients’ anti-HCV antibody test results between January 1, 2021 and December 31, 2023. The study included patients who were found to have reactive anti-HCV antibodies and were subsequently subjected to HCV-RNA PCR and HCV genotyping tests to confirm the presence of the HCV. In the case of repeated samples from the same patient, only the results at admission were included in the study, and repeated samples were excluded. The results of the virological tests were analyzed in conjunction with the demographic data. The analysis results were obtained from the Laboratory Information System (LIS). The patient’s demographic data (age, gender, year) were obtained from the hospital database. However, it was not possible to test the accessibility of patients to treatment. Furthermore, the prevalence of co-infection with HCV was investigated in patients who were HIV-positive by PCR.
Our hospital serves approximately 1 million people in the region. In addition, samples with high HCV risk are tested from the Sincan Prison Enforcement Institutions Campus, the second largest prison campus in Turkey. This prison has a capacity of 6830 detainees and convicts in an area of 2,500,000 m² and thirteen penal execution institutions with L and F-type security levels.
The Analysis of Anti-HCV Antibodies
Anti-HCV and anti-HIV testing was conducted using two distinct serological devices. The anti-HCV tests were conducted using the Architect anti-HCV kit (Abbott Laboratories, USA) and the MAGLUMI Anti-HCV (Snibe, Shenzhen, China) device (15).
The Quantitative Analysis of HCV RNA
Viral nucleic acid isolation was performed with QIAsymphony DSP virus/pathogen midi kit (Qiagen, Germany) and QIAsymphony SP/AS (Qiagen, Germany), and the polymerase chain reaction (PCR) was performed by using Artus HCV QS-RGQ (Qiagen, Germany) kit and Rotor-Gene Q (Qiagen, Germany).
HCV Genotyping
The Qiagen HCV genotyping kit (Qiagen, Germany) can detect and characterize the GT (by sequence analysis method) of HCV in human serum or plasma. It can identify six major and most predominant HCV GTs (GT1, GT1a, GT1b, GT2, GT3, GT4). The results were evaluated in accordance with the manufacturer’s recommendations for the kit. The analytical sensitivity of the Qiagen HCV genotyping kit was determined to be 1×10² IU/mL.
HIV Co-Infection
HCV/HIV co-infection was analyzed in patients with positive Geenius HIV-1/2 (Bio-Rad, Redmond, WA, USA) confirmation by national public health.
Statistical Analysis
The statistical analyses were performed by the Statistical Package for Social Sciences (SPSS) 25.0 (IBM Corp., Armonk, NY, USA). The median, interquartile range (IQR), minimum and maximum values for continuous variables were calculated. The counts and percentages were calculated for categorical variables. The data were tested for normal distribution using the Kolmogorov-Smirnov and Shapiro-Wilk tests. The Mann-Whitney U test and the Kruskal-Wallis test were employed to assess the statistical significance of numerical variables, while Pearson’s Chi-square and Fisher’s exact tests were used to analyze the statistical relevance of categorical variables. The odds ratio (OR) was calculated using the relevant basic formulas. The statistical significance was set as p<0.05.
Results
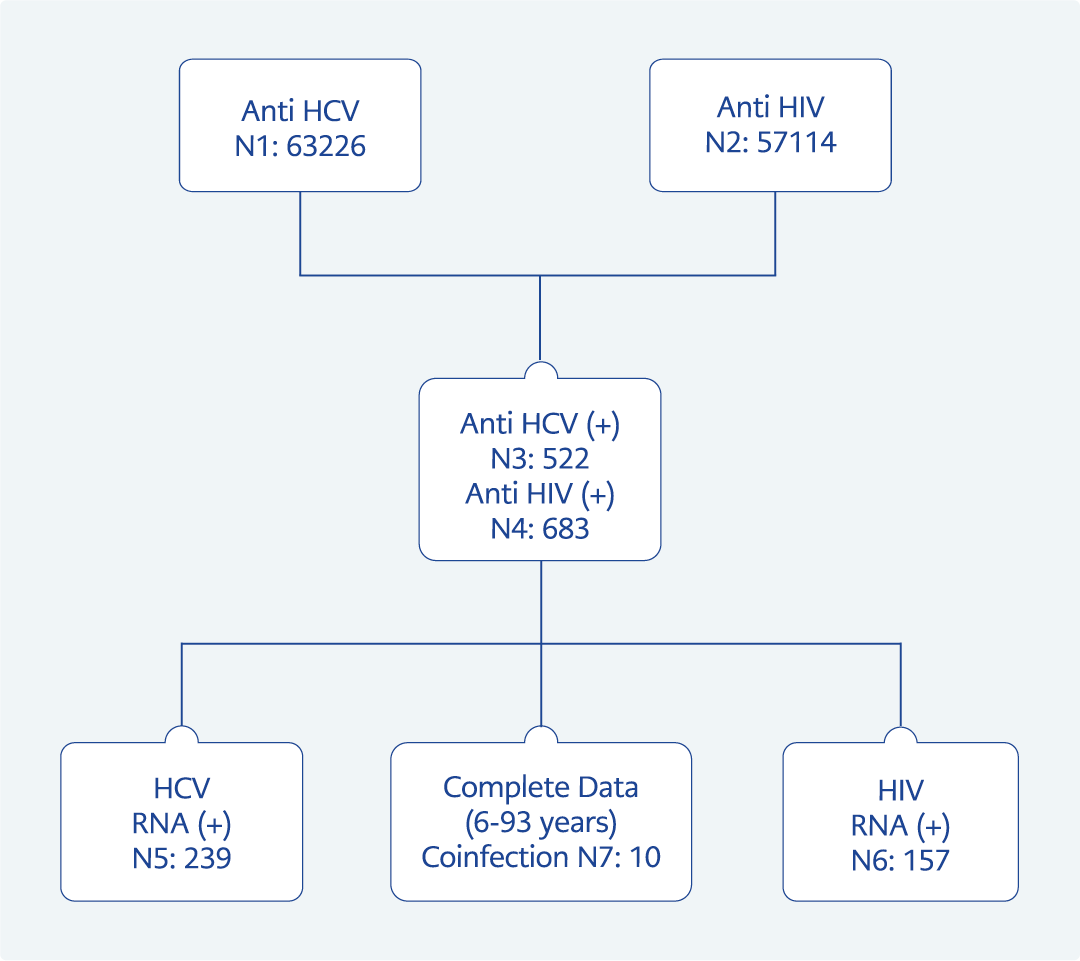
Figure 1. Flowchart of HCV and HIV testing, antibody positivity, and RNA detection rates.
A total of 63,226 anti-HCV antibody tests were performed from January 1, 2021 to December 31, 2023, and the results of 522 patients were found to be reactive (HCV antibody positivity prevalence 0.8%) (Figure 1). During the same period, 7892 samples from the prison population were tested. The prevalence of anti-HCV among prisoners in 2021, 2022, and 2023 was 3.8% (92/2419), 4.2% (85/2090), and 2.7% (93/3383), respectively. The ages of 522 patients (68.9% male, 31% female) who underwent HCV GT testing ranged from 6 to 93 years, with a median age of 33 years (IQR=19-44). It was established that 267 (51.1%) patients with positive serological test results had been admitted from the penitentiary. The prevalence and rate of HCV viremia were determined as 0.4% and 45.7%, respectively.
Prevalence
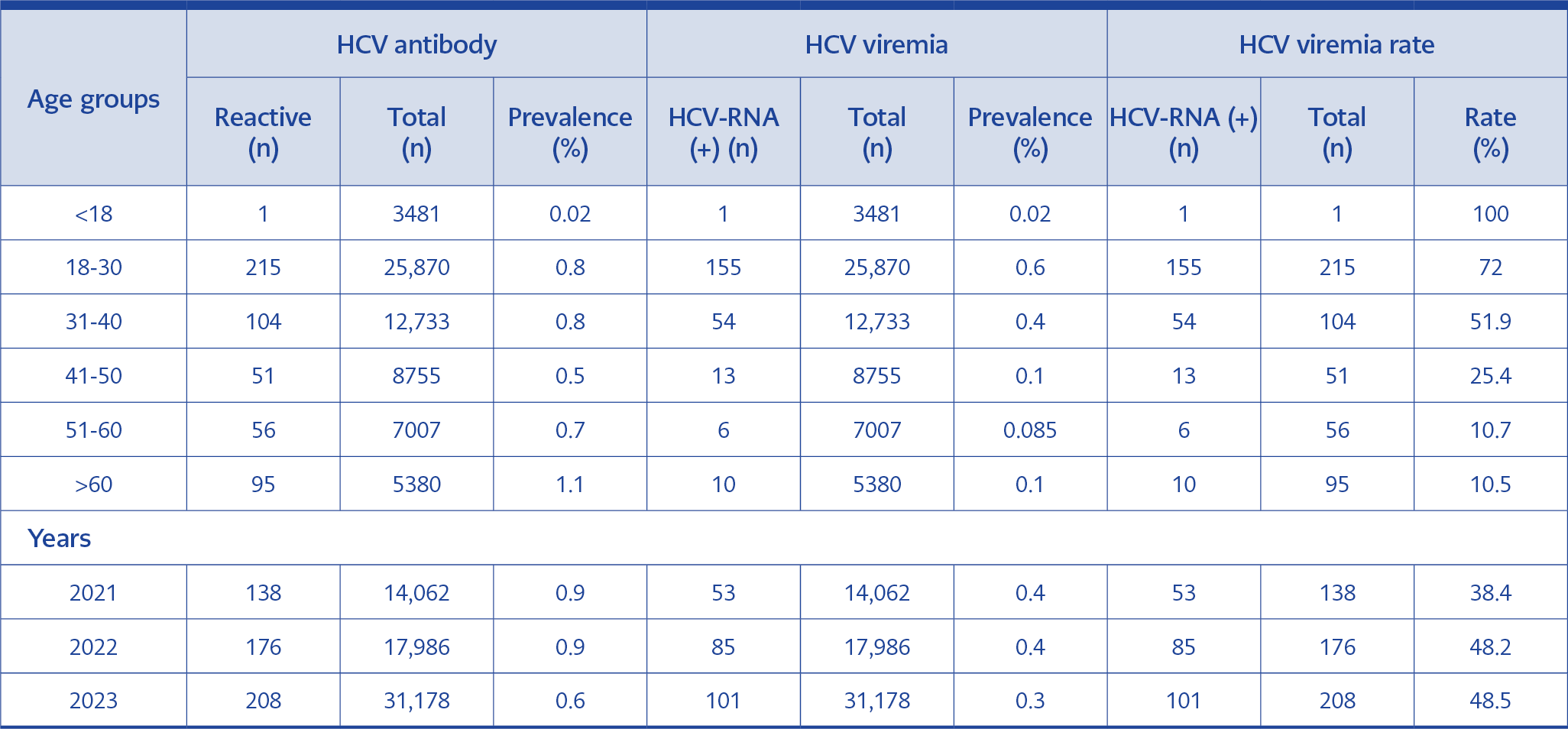
Table 1. The prevalence of HCV antibodies and viremia, and the distribution of HCV viremia rates by age groups and years.
HCV-infected patients were categorized into six age groups (0-18, >18-30, 31-40, 41-50, 51-60, and >60 years). The prevalence of viremic HCV infection showed different variations with age. The lowest prevalence was in the <18 years age group (0.02%), and the highest prevalence was in the 18-30 years age group (0.6%). HCV antibody prevalence detected in 2021 and 2022 (0.9%) was higher than in 2023 (0.6%). No significant difference was observed in the prevalence of HCV antibodies across the years. The HCV viremia rate was found to be 38.4 and 48.2, respectively, in 2021 and 2022, while the HCV viremia rate was detected to be the highest at 48.5% in 2023. A total of 32,048 HCV antibody levels were tested in 2021 and 2022, while 31,178 patient samples were studied in 2023. The prevalence of HCV antibodies and viremia and the distribution of HCV viremia rates from 2021 to 2023 are presented in Table 1.
Four HCV GTs (1-4) and two GT1 subtypes were investigated in 239 patients’ samples (Figure 1). HCV GT3 (27.9%) was found to be the most common GT, and this was followed by GT1 (26.2%), GT2 (7%), and GT4 (4.1%). Subtype 1b was detected in 36.5% of patients, and subtype 1a was detected in 33.3%, while the subtype could not be determined in 30% of the samples. Infection with a single HCV GT was identified in 65.6% (157/239) of the patients. No instances of mixed infection were identified in any samples.
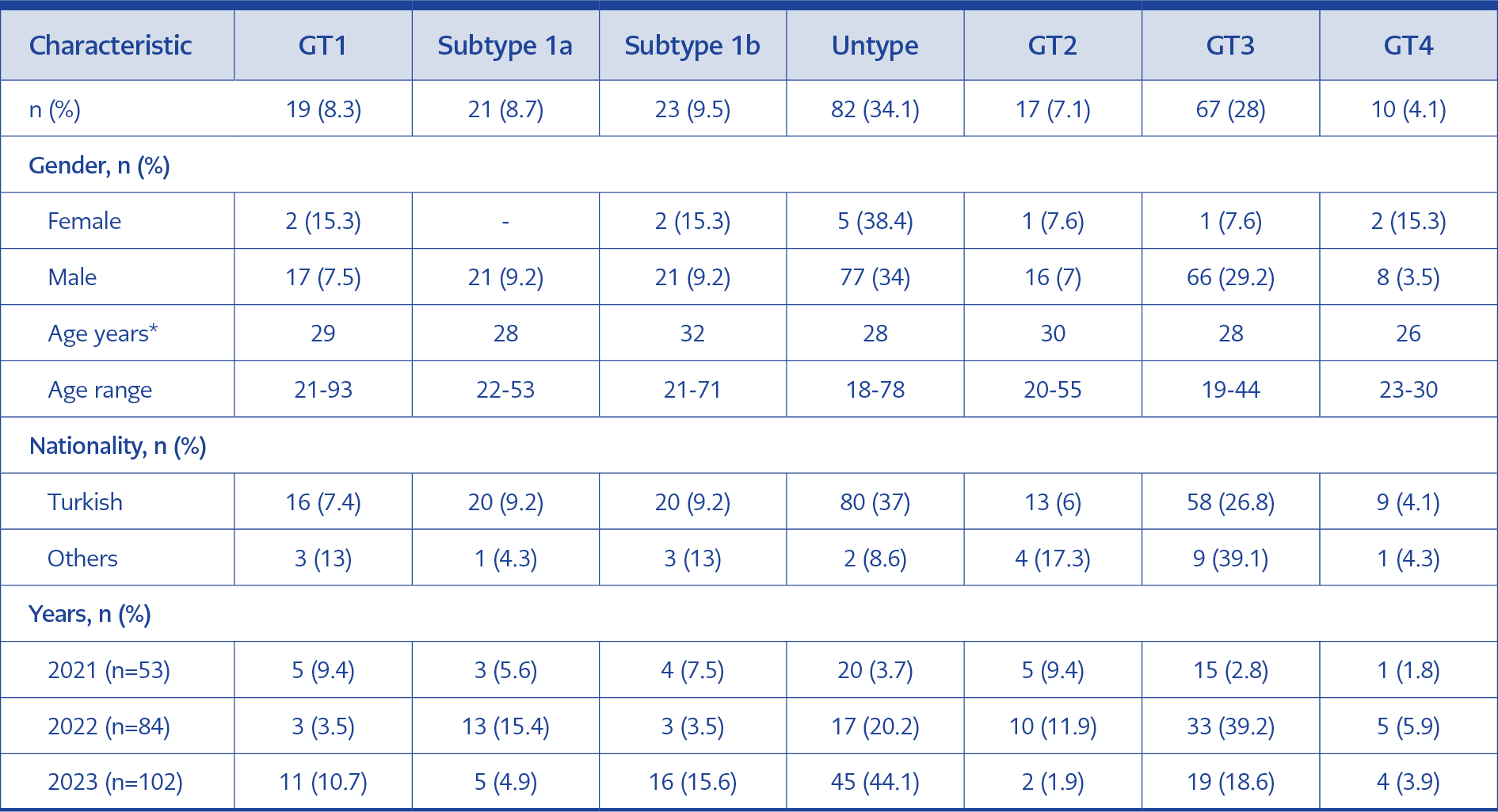
Table 2. Distribution of HCV genotypes in the studied population.
The GT3 was the predominant GT among the male participants, accounting for 29.2% of the cases (226 males, p<0.001), whereas GT1, subtype 1b, and GT4 were the most frequent GTs among the female participants, with 15.3% (13 females). The prevalence of GT3 was higher in males (29.2% vs. 7.6%), while GT4 was more common in females than males (3.5% vs. 15.3%). The distribution frequency of HCV GTs among different sex groups is shown in Table 2. No significant difference was found between median ages according to GTs. Among those typified are GT3 was more common in male patients (29.2%, n=66, p<0.001), and GT1b, GT4, and GT1 was more common in female patients (15.3%, n=13).
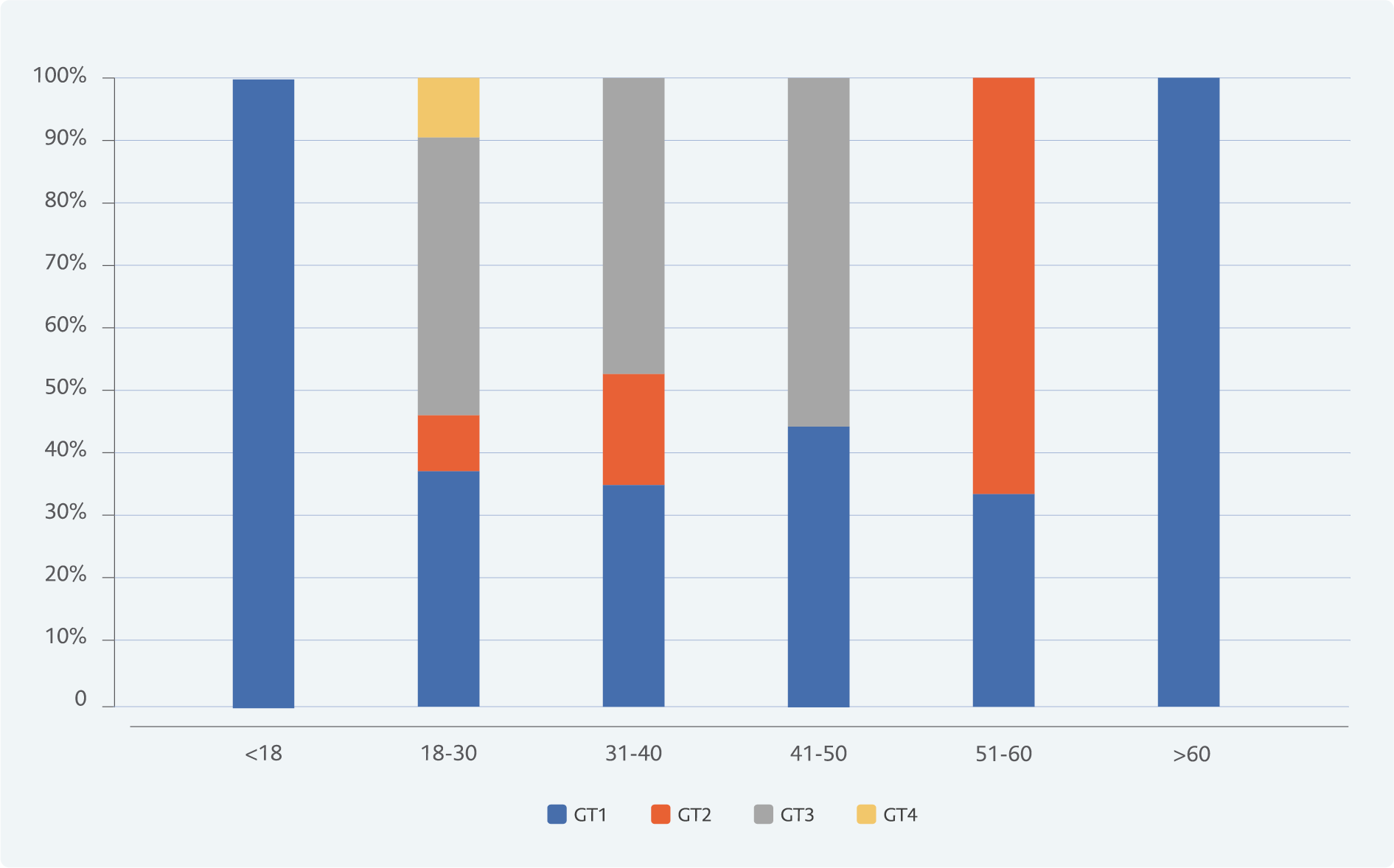
Figure 2. Distributions of different HCV genotypes (GTs) in different age groups.
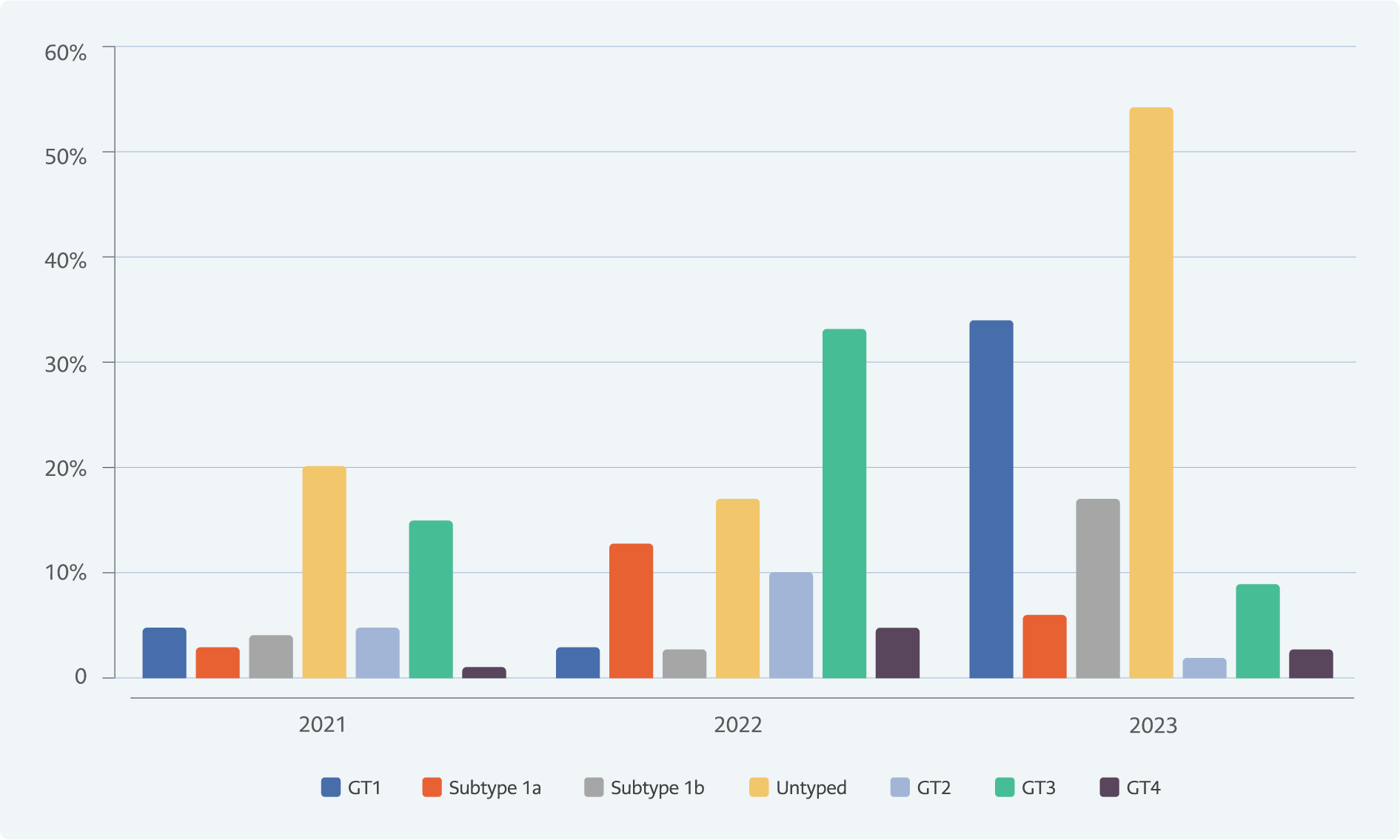
Figure 3. Yearly distribution of HCV genotypes and subtypes in the study population (2021–2023).
HCV GT distribution by age from January 2021 to December 2023 is presented in Figure 2. The median age of patients with GT4 was lower than those with GT1, GT2, and GT3. The distribution of subjects according to age group is as follows: GTs were GT3 in the 18-30 years age group (68.6%, n=46), the 31-40 years age group (23.8%, n=16) and the 41-50 years age group (7.4%, n=5). The prevalence of anti-HCV positivity (1.1%) was highest in people aged over 60 years. GT2 and GT1 were the most common GTs in the 51-60 (33.3%, n=2) and >60 years (66.6%, n=6) age groups, respectively. The only pediatric patient in the study was a female under 18 years old, and GT1b was detected. The change in HCV GTs over the years is given in Figure 3.
GT4 was associated with a higher viral load (median, 17.73×105), and GT3 (median, 5.1×104) was associated with a lower viral load. Although the viral load was higher within the non-classified group of GT1, no statistically significant difference was observed in the comparison of GT1a and GT1b groups.
HCV/HIV Co-Infection
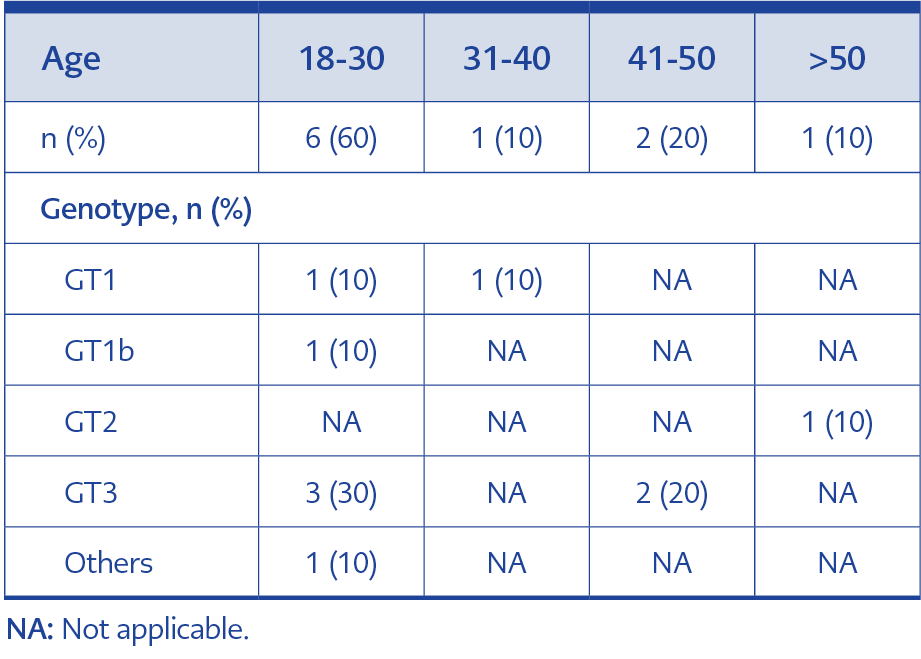
Table 3. Distribution of patients with HCV/HIV coinfection.
Between 2021 and 2023, 57,114 patients were analyzed for anti-HIV, and 683 cases were found to be reactive. There were 157 cases identified as positive by HIV confirmation. All ten patients with HCV viremia and HIV co-infection were male, with a median age of 28 years. The prevalence of HCV/HIV co-infection was 4.1% (n=10). Table 3 presents the characteristics of patients with HCV/HIV co-infection. When the GT distribution of co-infected patients was analyzed, GT3 (50%) was the most common, while five cases were foreign nationals.
Discussion
A total of 63,226 anti-HCV antibody tests were conducted, and the results of 522 patients were found to be reactive (HCV antibody positivity prevalence 0.8%). The prevalence and rate of HCV viremia were determined to be 0.4% and 45.7%, respectively. Patients infected with HCV were categorized into six age groups (0-18, >18-30, 31-40, 41-50, 51-60, and >60 years). The prevalence of viremic HCV infection demonstrated age-related variations.
The prevalence of HCV infection represents a significant challenge to global public health. The World Health Organization developed a plan in 2016 for eliminating viral hepatitis by 2030 (2). The Global Health Sector Strategy (GHSS) aims to reduce new HCV infections by 80% by 2030 (16). However, the emergence of the SARS-CoV-2 pandemic has made this goal extremely difficult to achieve due to a reduction in screening tests and strict lockdown measures.
The prevalence of HCV infection is influenced by several factors, including the country’s geographical location, population mobility (such as travel and migration), and socioeconomic status. The prevalence of HCV infection is less than 2% in developed countries and up to approximately 15% in developing countries (2).
A comprehensive registry database that could provide an accurate overview of the prevalence of HCV infection in Türkiye does not currently exist. The majority of epidemiological data is derived from local studies. In population-based studies, the prevalence of anti-HCV antibodies in the general population was found to range from 0.4 to 2.1%. Nevertheless, in blood donors, this rate was reported to be between 0.19 and 0.68% (17).
HCV prevalence and treatment rates are low in Türkiye. A study reported that the prevalence of HCV infection in our country was 16%, and the estimated treatment rate was 0.8% (18). A 2014 meta-analysis study evaluating the global prevalence of HCV viremia revealed that the prevalence of HCV viremia in North Africa and the Middle East ranged between 0.4% and 10%. The prevalence of HCV viremia was found between 51.6% and 81.8% (17). In a study conducted in our country, the prevalence of anti-HCV positivity and viremia was found to be 2.24% and 0.67%, respectively (18). HCV-RNA test was requested from 71.7% of anti-HCV positive patients, and it was also reported that 44.4% of viremic patients were not given antiviral treatment (19). In another study, it was estimated that 10,200 of 271,000 viremic patients (approximately 38%) were treated, and (99%)10,100 of those who received treatment recovered (20). GT1 was the most prevalent genotype worldwide, accounting for 46-49% of all HCV infections. GT3 followed closely behind, with a prevalence of 17.9-30%. GT2, GT4, and GT6 collectively accounted for 22.8% of all cases, while GT5 represented the remaining <5% (21, 22).
Several studies have been conducted to elucidate the distribution of HCV genotypes for chronic hepatitis in our country. A previously published study revealed that GT1b was the predominant genotype, accounting for 52.8% to 87.5% of cases (23). Yaman et al. conducted a study investigating the prevalence of HCV viremia and genotype distribution in Turkish citizens and immigrants. The authors reported a prevalence of 0.5% for HCV antibody positivity and 0.1% for viremia. While GT1 (65.1%) was the most prevalent genotype among Turkish citizens, GT4 (52.3%) was the most common genotype among immigrants, predominantly of Syrian and Ukrainian origin (23). However, the distribution of genotypes may vary between different geographical regions within a country. A regional analysis of GT distribution was performed in another study conducted in our country. GT3 was the most frequently observed genotype, accounting for 44.1% of the cases; it was followed by GT1a (41.9%), GT2 (5.1%), GT4 (4.4%), and GT1b (4.4%) (24). Furthermore, the most common GT in the Central Anatolia region of Türkiye (the region where our hospital is located) was GT3, with a frequency of 44.4%. It was reported that the frequencies of GT1a and GT3, which were detected predominantly in the south and northwest regions of Türkiye, were very close to each other (24). Another study by Cırıt et al. analyzed data from 1628 patients. It was demonstrated that GT1 was present in 51.5% of cases, GT3 in 21.4%, GT4 in 20%, GT5 in 4.6%, and GT2 in 1.3%. A total of 20 patients exhibited a mixed genotype. Among 1143 Turkish patients, GT1 (66.8%) was the most prevalent genotype, followed by genotype 3 (29%). Among the Syrian patients (n=477), the predominant GT was GT4 (64.2%), followed by GT1 and GT5. GT3 was identified in 277 (79.6%) prisoners (25). The ethnic differences of immigrants or the socio-demographic status of the region may affect the GT distribution (23, 28).
Similar to the literature, we found GT3 (28%) to be the most prevalent genotype. GT3 was followed by GT1 (26.2%), GT2 (7%) and GT4 (4.1%) in our study. The prevalence of GT3 can be attributed to the fact that most of the cases observed were those of prison inmates. We believe that the untyped genotype, which has increased in recent years, is now only associated with pan-genotypic agents in Türkiye.
HCV and HIV viruses are pathogens with common transmission routes. Liver damage, and mortality and morbidity rates are high in the case of HCV/HIV co-infection (26). A study on HCV/HIV co-infections has indicated that end-stage liver disease (such as cirrhosis) occurs at an earlier stage in patients co-infected with HCV and HIV, in addition to increased levels of ALT and AST compared to patients with HCV infection alone (12). Another study found the rates of HCV/HIV co-infection ranging from 1.6% to 74% with a considerable variation (14). The prevalence of co-infection in our study was 4.1%. Comparable to our findings, another study found the HIV/HCV co-infection rate 6.9% (27).
Our study has some limitations. Firstly, because of its retrospective design, transmission routes and risk groups could not be evaluated in patients; also, nucleotide sequencing could not be performed. Second, it represents a single center’s experience and does not reflect the whole country. Third, subtype definitions are limited because of the test kit design we used. Nevertheless, our findings can contribute to the understanding of the epidemiological landscape of HCV infection and its co-occurrence with HIV in Ankara, Türkiye. Also, it can contribute to the development of tailored public health interventions and optimized treatment strategies to address the burden of HCV and HIV co-infection in the region.
In conclusion, alteration in Türkiye’s demographic structure due to the recent population movement may cause a change in the distribution and prevalence of HCV genotypes. Therefore, further studies are needed to ascertain the GT profile of HCV, determine the prevalence of HCV and HIV co-infections, monitor the clinical process, and evaluate treatment outcomes.