Introduction
Henoch-Schönlein purpura (HSP) is a systemic small-vessel vasculitis characterized by involvement in the skin, kidney, and gastrointestinal system. It is frequently seen in children, accounting for 90% of cases. HSP is less common in adults (1). Cutaneous involvement is the most common presentation, and in some cohorts, adult HSP is more severe and has worse renal outcomes (2, 3).
AIDS is a viral infection that can be associated with the development of serious opportunistic infections and malignancies. Furthermore, it can give rise to inflammatory and autoimmune diseases. Vasculitis is very rare in human immunodeficiency viruses (HIV) infection, with an incidence of <1% reported in the literature (4). HSP has also been rarely reported in people living with HIV. In this paper, we reviewed the relevant literature and presented a case of HSP in a patient with acquired immune deficiency syndrome (AIDS).
Case

Figure 1. Symmetric purpuric papules involving extremities and abdomen.
A 27-year-old man presented with a fever and a widespread purpuric rash that had persisted for four days. He had been diagnosed with HIV infection in 2018 but was not receiving antiretroviral therapy (ART). The rashes did not fade with pressure and were distributed throughout the body, commonly affecting the palmoplantar regions of the hands, trunk, and bilateral extremities (Figure 1). There was transient or migratory joint pain involving the hips and knees. They were remarkable for tenderness without erythema or warmth. He had a documented high fever (38.2 °C), and a physical examination revealed the presence of bilateral painless cervical, axillary and inguinal lymphadenopathies ranging from 15 mm to 32 mm in size (LAPs) and splenomegaly (272 mm in size). He denied recent drug use for an allergic condition and a genital ulcer. A wide variety of differential diagnoses, such as lymphoma, tuberculosis, HIV infection itself, Castleman disease, and syphilis, were primarily considered.
Laboratory studies revealed pancytopenia with a hemoglobin level of 6.9 g/dL, a white blood count of 3600/mm3 and a platelet level of 86,000/mm3, erythrocyte sedimentation rate of 58 mm/hour, C-reactive protein (CRP) 120 mg/L. In the report, a peripheral blood smear revealed platelet level >50,000/mm3, rulo formation, hypochromic microcytic anemia suggesting anemia of chronic disease, and no atypical cells. He had chronic HBV infection (HBsAg positive, HBV-DNA <2000 IU/mL). Both the venereal disease research laboratory (VDRL) test and the VDRL titers were negative, but the treponema pallidum hemagglutination (TPHA) test was positive. HIV-1 RNA level was 123,000 copies/mL a with a low CD4+ T lymphocyte count of 137 cells/dL.
ART, including bictegravir/tenofovir alafenamide/emtricitabine, was administered on the sixth day of admission. A serum cryptococcal antigen test was negative. The levels of creatine phosphokinase, cryoglobulin, antinuclear antibody, cytoplasmic- antineutrophil cytoplasmic antibody (c-ANCA), perinuclear-ANCA (p-ANCA), rheumatoid factor, anti-cyclic citrullinated peptides (anti-CCP), and extractable nuclear antigen antibodies were within the normal limits. Serum complement C3 and C4 levels were normal. The initial urinalysis, transaminases, total bilirubin, haptoglobin and lactate dehydrogenase were within normal ranges. Baseline serum creatinine level 0.7 mg/dL and glomerular filtration rate (GFR) level 129 mL/min/1.73 m2. Parvovirus B19 IgG was positive, and the ferritin level was 924 µg/L.
The lesions were examined by a dermatologist and rheumatologist, with vasculitis being the primary consideration. A skin biopsy from the lesions showed an accumulation of IgA, C3 and fibrinogen in the vessel wall by direct immunofluorescence, suggesting HSP. Gastrointestinal endoscopy, colonoscopy and echocardiography of the patient were normal. The ophthalmic examination was unremarkable. F-18-fluorodeoxyglucose positron emission tomography/computed tomography (F-18 FDG PET/BT) revealed generalized reactive lymphadenopathies with low FDG uptake, suggesting secondary to HIV infection in the report. Biopsies of lymphadenopathy and bone marrow were made due to additional pathological findings.
Subsequently, a daily dose of 250 mg of methylprednisolone was administered for three days, after which the dosage was tapered off. Following the administration of steroids and ART, the patient’s fever abated, and the rashes gradually resolved. An excisional biopsy of the inguinal lymph nodes was found to be compatible with Kaposi sarcoma (KS). The material was re-evaluated for the presence of Castleman’s disease, but this was not considered by the pathologist. On examination of the bone marrow biopsy, the abnormalities were considered to be secondary to HIV infection. On subsequent follow-up, the patient’s condition deteriorated, with recurrent fever. Multiple organ dysfunction was developed.
Serum urea concentration of 95 mg/dL, serum creatinine level of 1.9 mg/dL, and aspartate aminotransferase of 68 IU/L (normal 0-50), alanine aminotransferase of 20 IU/L (normal 0-50), gamma-glutamyl transferase of 154 IU/L (normal 0-38), alkaline phosphatase of 40 IU/L (normal 30-120), total bilirubin: 13.9 mg/dL, with a direct fraction of 12.9 mg/dL and international normalized ratio (INR) 2.4, CRP 288 mg/L, procalsitonine 46 µg/L, plenty of leukocytes were seen in the urinalysis. After taking two sets of hemocultures, meropenem 3×1 gram, a loading dose of teicoplanin and fluconazole 1×400 mg were empirically initiated. Chemotherapy was not considered by an oncologist due to the patient’s poor condition. All hemocultures remained sterile. On day 16th of ART, he died of multiple organ failure in the hospital.
Discussion
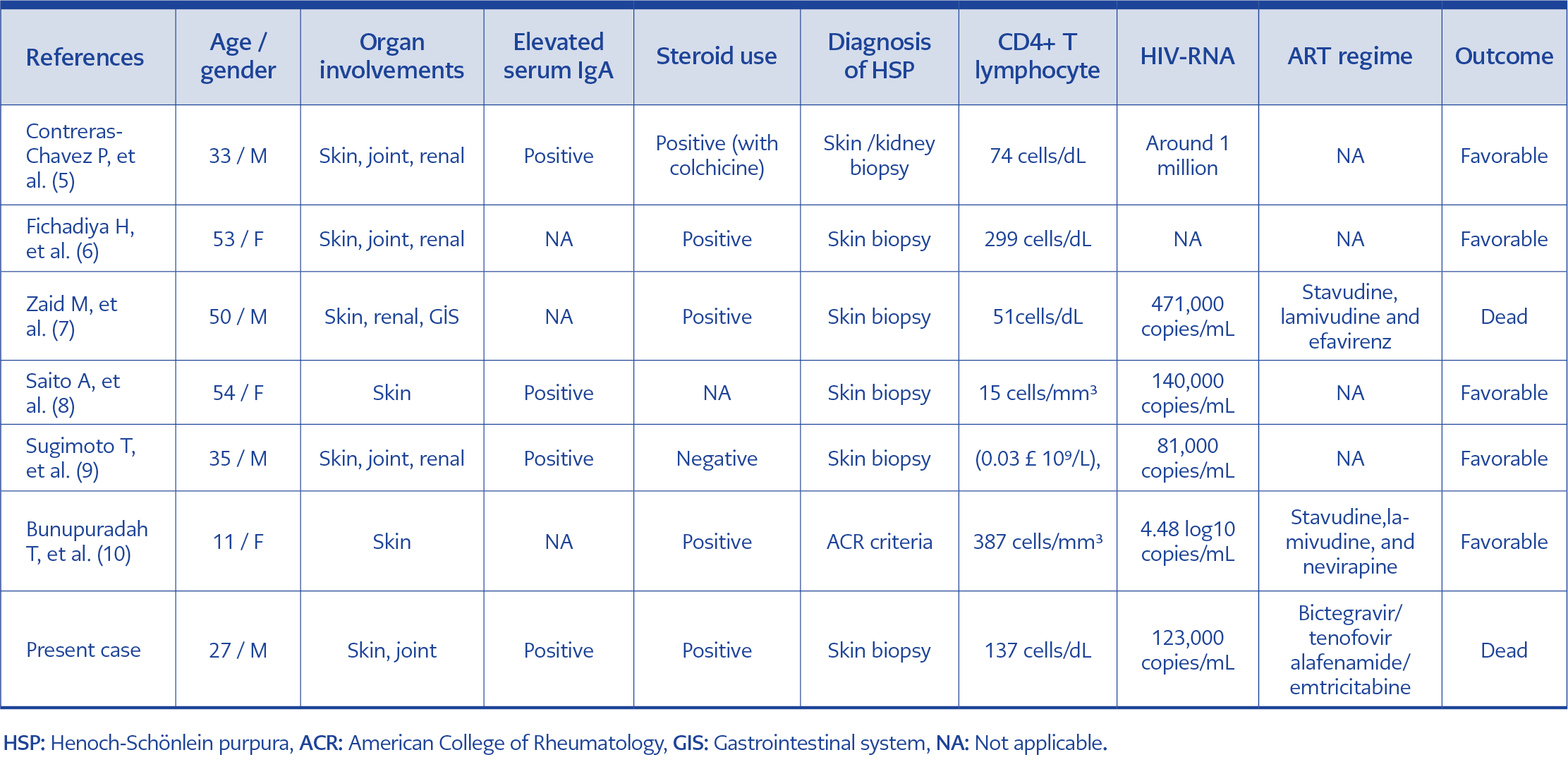
Table 1. The characteristics of all patients.
HSP is an extremely rare condition in people living with HIV, and six well-documented cases were reported in the English literature (5-10). The characteristics of the patients, including our report, are shown in Table 1. Three of them were female, and the mean age was 37.57 (range=11-54 years). One was a child. All cases had skin involvement. Elevated serum IgA was found in all patients tested. In most cases, the diagnosis was made by a skin biopsy or skin+renal biopsy (in one case) in addition to the fulfilment of rheumatological criteria (one patient). Five of six patients had a markedly decreased CD4+ T lymphocyte count (<200 cell/mL), and three were on an ART regimen. Steroids were administered to five patients, with one case receiving them in combination with colchicine. Two cases died from complications. In a study of 98 HIV-positive patients conducted by Zhang et al., two cases of HSP were observed (4). In their study, patients with HIV and rheumatic complications were most often observed in the advanced stage (40/53 cases, 75.47%). In another study by Lordache et al., 52 patients with HIV were reviewed; three of these patients had HSP, and two had CD4+ T lymphocyte count <200 cell/mL (11). These studies were not included in the table because of insufficient patient data.
The clear cause of vasculitis in patients living with HIV is not completely elucidated. These patients may also develop vasculitis due to co-infection with other viruses (hepatitis B virus, hepatitis C virus, parvovirus B19, Epstein-Barr virus), opportunistic infections (Pneumocystis jiroveci, cytomegalovirus, varicella zoster virus and Toxoplasma gondii), and drug-induced hypersensitivity (12). A number of theories have been postulated for this: 1) the direct effect of HIV on vascular wall injury, 2) immune complexes or autoantibodies, 3) cell-mediated toxicity, and 4) immune reconstitution inflammatory syndrome during ART (4, 13). The mechanism of HSP is still unknown in HIV patients. Several factors, such as infections, medications, vaccinations and their combinations, were reported as possible triggers for HSP (4).
In our case, the development of HSP may be caused by HIV and HBV co-infection. It is also known that solid tumors can act as a trigger factor for HSP in approximately 5% of cases, and non-small cell lung cancer is the most common cancer associated with HSP (14). On the other hand, the presence of primary lymph node KS and KS without skin involvement were interesting features in our patient. Both are rare in the literature, with only a few documented cases (15). In this patient, HSP may also be caused by Kaposi’s sarcoma-associated herpesvirus (KSHV) / human herpesvirus type 8 (HHV8 ). In HIV patients, the effective therapy and the role of steroids in HSP is unclear, and more reports are needed to clarify.
Although the incidence and mortality associated with KS have decreased with the use of ART, it remains the most common malignancy in HIV-infected populations (16). The risk of developing KS is increased with lower CD4+ T lymphocyte counts and higher HIV viremia. However, it can be seen in patients who are well-controlled on ART and have a preserved CD4+ T lymphocyte count (17). In HIV patients, corticosteroids are frequently used for P. jiroveci infections, tuberculous (TB) meningitis and TB-immune reconstitution inflammatory syndrome (TB-IRIS). However, the use of corticosteroids has been associated with the development of KS and worsening of KS and KS-IRIS (18). Also, they increased KS-related mortality in the HIV-infected population. Therefore, clinicians should be aware of this condition.
In conclusion, rheumatic manifestations such as HSP in patients with HIV are rare clinical conditions but can even be fatal, as in our patient. In such cases, there is no clear consensus on the treatment, and the use of steroids is controversial. The prompt initiation of ART may yield better outcomes in these patients.