Introduction
Healthcare-associated infections (HAIs) are accepted as one of the most important challenges in hospital settings. They cause extended lengths of stay -at the hospital, threatening patient safety, increasing the rate of morbidity and mortality, raising the workforce of healthcare workers and accelerating antimicrobial resistance (1). According to the World Health Organization (WHO), HAIs are accepted in the most common three hospital complications with drug errors and surgical complications (2-4). The European Centre for Disease Prevention and Control (ECDC) reported that more than 3.5 million people get HAI diagnoses, and more than 90 thousand patients lose their lives annually. Moreover, 71% of these infections are multidrug-resistant (5). The devastating impact of HAI is more dramatic in low-middle-income countries than in high-income countries (6, 7). According to the literature, for every seven patients getting HAI diagnosed in every 100 inpatients in developed countries, this rate has risen to 10 in developing countries (8). While the rate of HAIs is changing between 5% and 15% in inpatient wards, it rises to 37% in intensive care units (ICUs) (4, 9).
A regulation for the systematic surveillance of HAIs was implemented in 2005 by the Republic of Türkiye Ministry of Health. According to the regulation, every healthcare center should report its HAI rates. However, there has been no overall evaluation report of this process up to now. Therefore, we aimed to review the published reports on HAIs in Türkiye to describe the current situation, detail gaps, and deliver future research topics.
Materials and Methods
Study design, registration, and search protocol
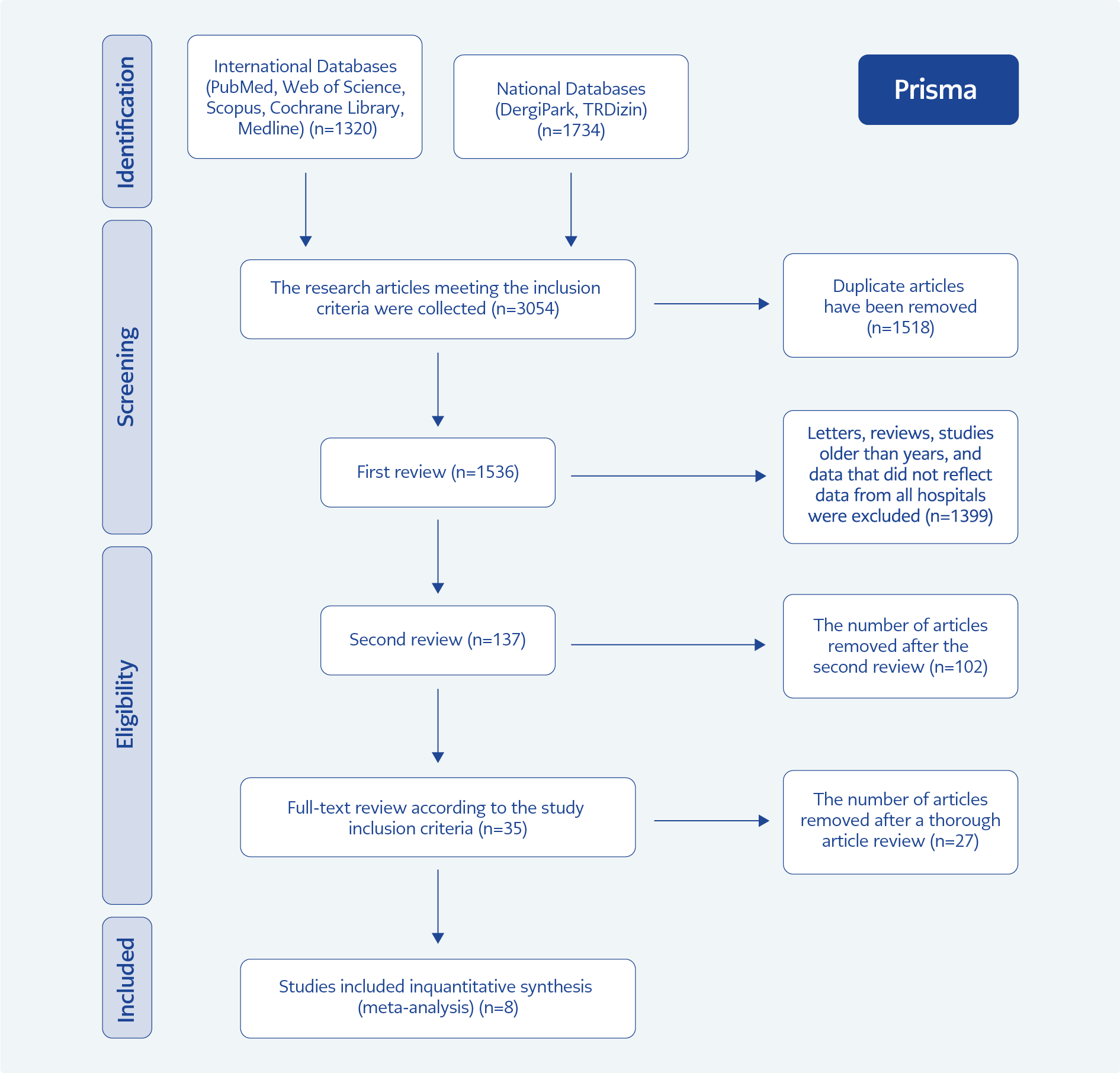
Figure 1. Flowchart for selection of the study reports.
We followed the steps of the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) checklist statements (Figure 1). A librarian searched articles published from January 01, 2014, to December 31, 2023, using PubMed, Web of Science, Scopus, Cochrane Library, Medline, DergiPark, and TRDizin (Supplementary 1) for the search strategy, which included variations of the following terms “Turkey” OR Turkey OR Türkiye AND “Bloodstream Infection” OR “Surgical site infection” OR “Surgical Wound Infection” OR “Pneumonia, Ventilator-Associated” OR “Ventilator-Associated Pneumonia” OR “Urinary catheter-associated infection” OR “nosocomial infection” OR “Cross Infection” OR “Healthcare-Associated Infections” OR “Hospital Infection” OR “Healthcare-Associated Pneumonia” OR “Nosocomial Pneumonia” OR “Hospital Acquired Pneumonia” OR “Cross Infection” OR “intensive care infection”.
Study selection and data collection
There were two phases of the selection process. In the first phase, two reviewers (B.M. and Z.A.) independently screened the titles; in the second phase, two researchers (E.S.A. and Ş.M.) were included in the abstract and full-text screening. We excluded the surveillance reports conducted with only pediatric inpatients, studies that do not reflect all surveillance data of the hospital, less than one year of data, and studies conducted in 2014 and before. The studies with promising titles, however, missing abstracts, were included in the full-text screening. The discrepancies in the selection were resolved via a consensus meeting among the research team.
Data from each article are based on the detailed results of HAI surveillance (The rate of central line-catheter-associated bloodstream infections [CLABSI], catheter-associated urinary tract infection [CAUTI], ventilator-associated pneumonia [VAP], other HAIs, the number of devices, the number of inpatients, the method of research, gender distribution, the mean age) carried out in ICUs and inpatients’ wards.
Risk of bias assessment
Systematic errors in each study were assessed for risk of bias (RoB) by one researcher (B.M.) using the Joanna Briggs Institute (JBI) critical appraisal tools. It is a 9-point scale where a score of 8-9 indicates a low RoB, whereas a score of 5-7 indicates moderate and <4 indicates a high RoB. While evaluating the RoB, we considered whether the definition of HAIs was made according to the international guidelines (ECDC, WHO, Centers for Disease Control and Preventions [CDC]) or the Ministry of Health guideline and whether the decision was approved by the infection control committee (Supplementary 2). As a result of RoB made after the evaluation of inclusion criteria, publications with high RoB were excluded from the study to prevent inappropriate studies.
Data analysis
The primary outcome measure was a pooled rate of HAIs obtained from articles. Heterogeneity between studies was assessed with the I2 statistic. Meta-analysis of the rates of HAIs was done with both fixed and random effect models under logit transformation with the inverse variance method (sm= “PLOGIT”; method= “Inverse”; method.tau= “DL”). Statistical analyses were done using a meta package in R and visualized as Forest plots.
Results
Our literature review yielded 3050 reports in total. After removing duplicates, the first and second screenings were conducted according to the title and abstract, and we included 35 articles for full-text review (Figure 1). Some studies had a high RoB, while some did not reflect the total scores of their centers. After all evaluations, eight studies (10-17) met the eligibility criteria (Figure 1). According to the RoB assessment, four studies showed moderate RoB, and four showed low RoB (Supplementary 2).
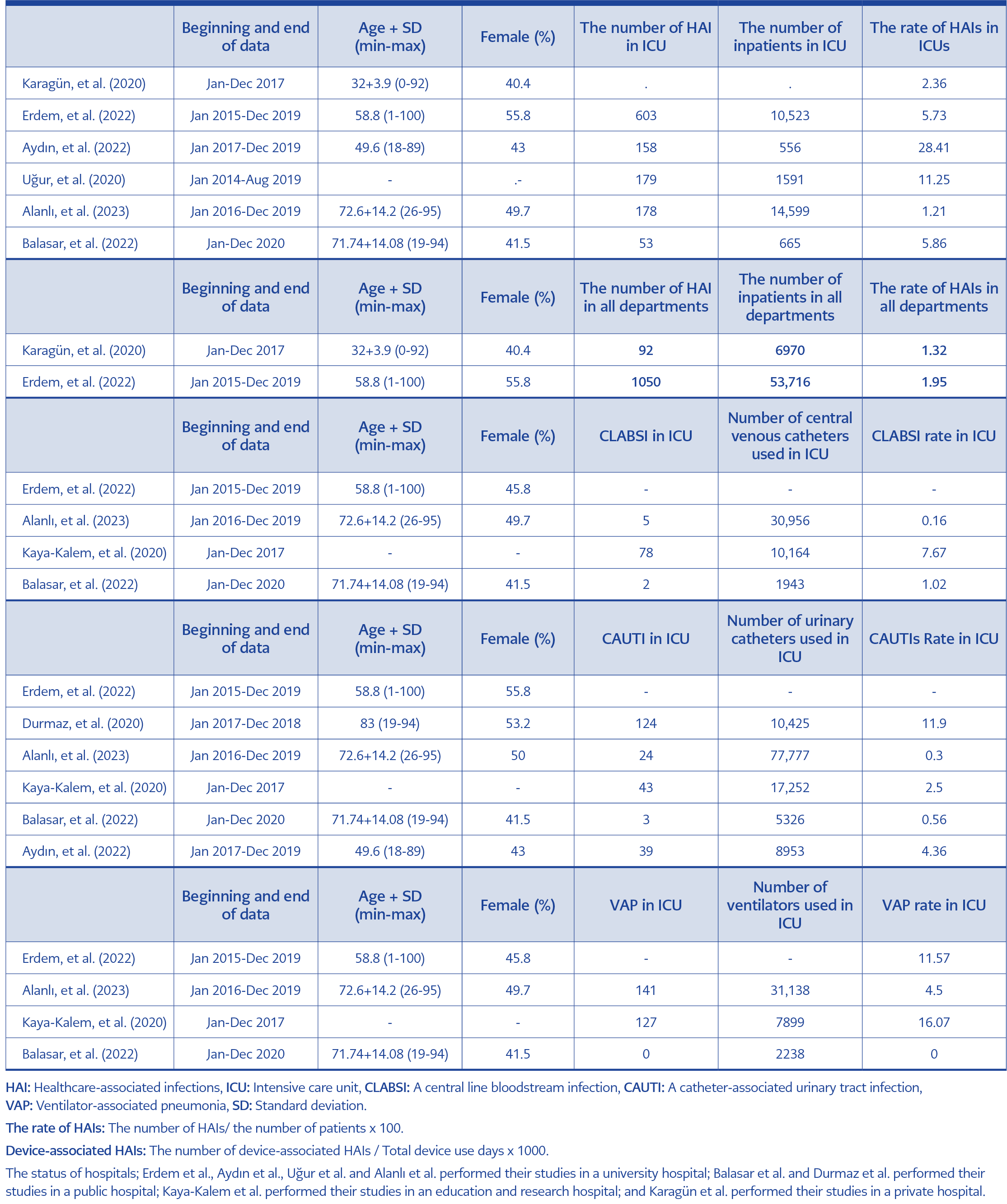
Table 1. The main characteristics of studies.
Table 1, which was grouped according to the HAI type, shows the studies’ main characteristics. The studies from January 01, 2014, to December 31, 2022, were included in the meta-analysis. The mean duration of data collection was 34 months (min. 12 months [12-16] and max. 68 months [17]). The range of mean age is 32 and 83. Four studies were performed in a university hospital, two in a public hospital, one in a private, and one in an education and research hospital.
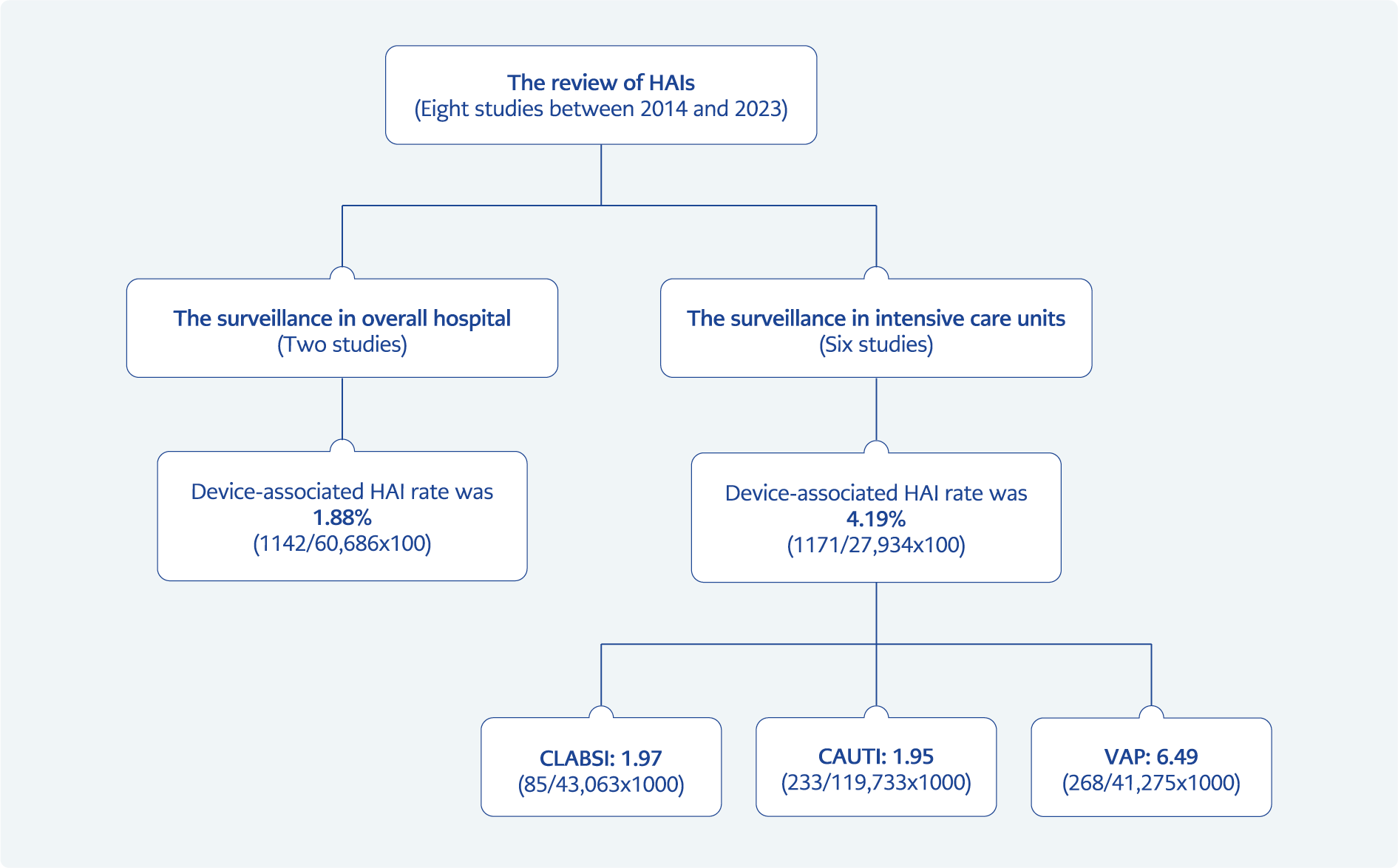
Figure 2. The rate of catheter-associated HAIs according to the surveillance in ICUs and overall hospital.
In total, data of 98,686 inpatients were included to calculate the overall rate of HAIs. The lowest patient number was 556 (12), while the highest was 53,716 (10) (Table 1) at the centers. The rate of overall device-associated HAIs was 4.19 (1171/27,934×100) in ICUs and 1.88 (1142/60,686×100) in inpatient wards. We evaluated 204,071 catheter usage days to assess the rate of catheter-related infections according to the type of catheter. As a result, the rate of CLABSI was calculated as 1.97 (85/43,063×1000), CAUTI was 1.95 (233/119,733×1000), and VAP was 6.49 (268/41,275×1000) in ICUs (Figure 2). Since no articles met the study inclusion criteria, we could not perform an analysis revealing the overall surgical site infection rate.
Discussion
Healthcare-associated infections are one of the major reasons for morbidity and mortality in healthcare settings. The Ministry of Health releases the annual reports of 1555 hospitals in Türkiye (18); however, the objectivity or transparency of the HAI rates that hospitals share with the Ministry due to performance concerns is often questionable. Therefore, our goal was to investigate the HAI rate in Türkiye in the last decade and compare the results with those of peer-reviewed journals.
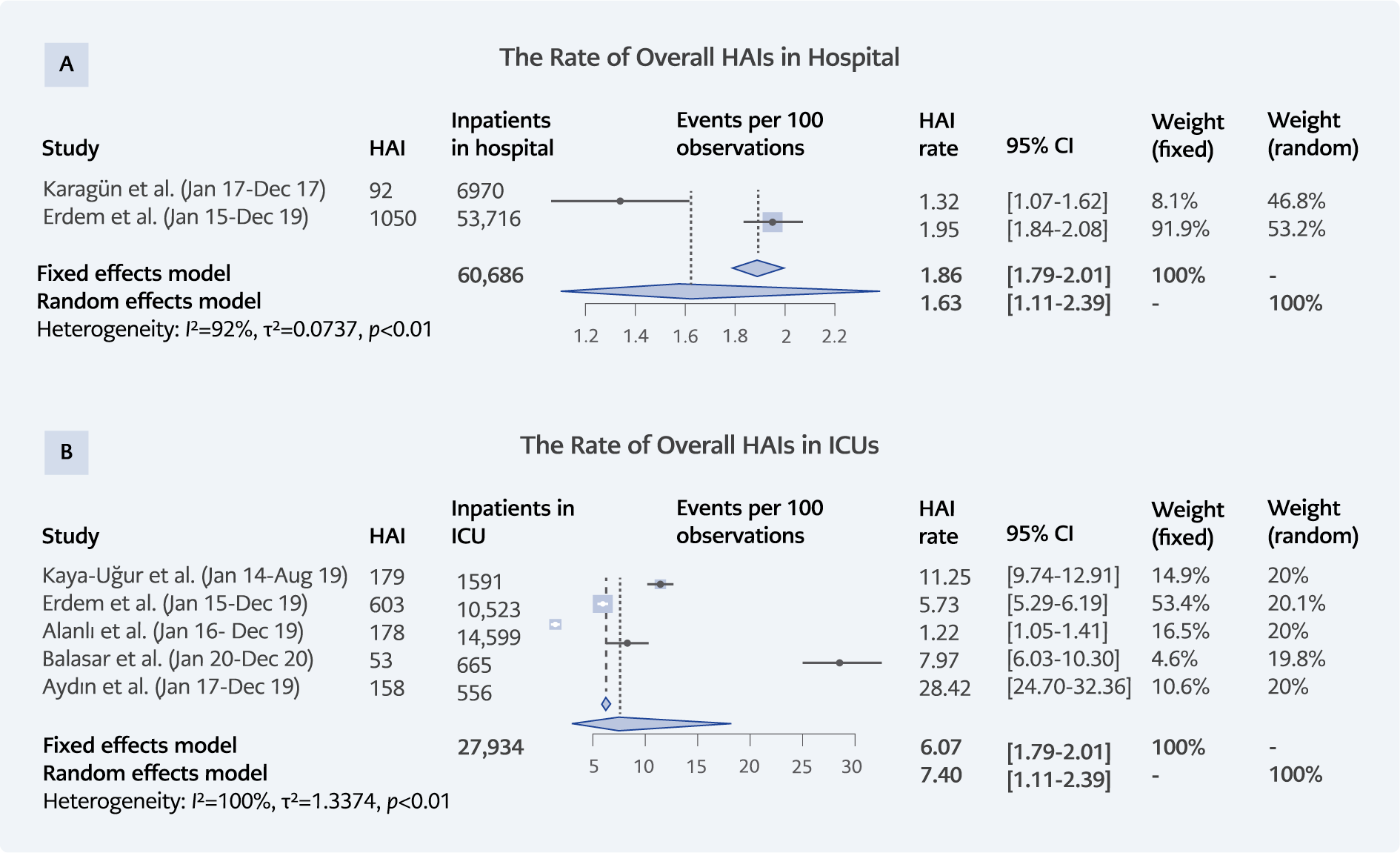
Figure 3. A. Forest Plot of the rate of overall HAIs of the result of the hospital surveillance in Türkiye. B. Forest plot of the rate of
HAIs of the results of the intensive care unit surveillance in Türkiye.
Our analysis showed that the overall device-associated HAI rate was 1.88% in hospitals and 4.19% in intensive-care units (ranging from 1.22 to 28.42) (Figure 3). No benchmark value from the Republic of Türkiye Ministry of Health reflects the general rate of HAIs in all hospitals. Europe released a rate between 3.9% and 6.5% in acute care hospitals and long-term care facilities (19). WHO revealed that the rate of HAI can reach up to 15% in low- or middle-income countries (20). Research findings show that up to 70% of HAIs can be prevented, but the risk of HAIs is still higher in patients due to lack of facilities, lack of training of healthcare workers or the population, and poor conditions in hospitals. Although the HAI rate results of our study are lower than those of other studies and reports, we believe that publication bias should be considered and that existing infection control strategies in our healthcare centers should be tightened.
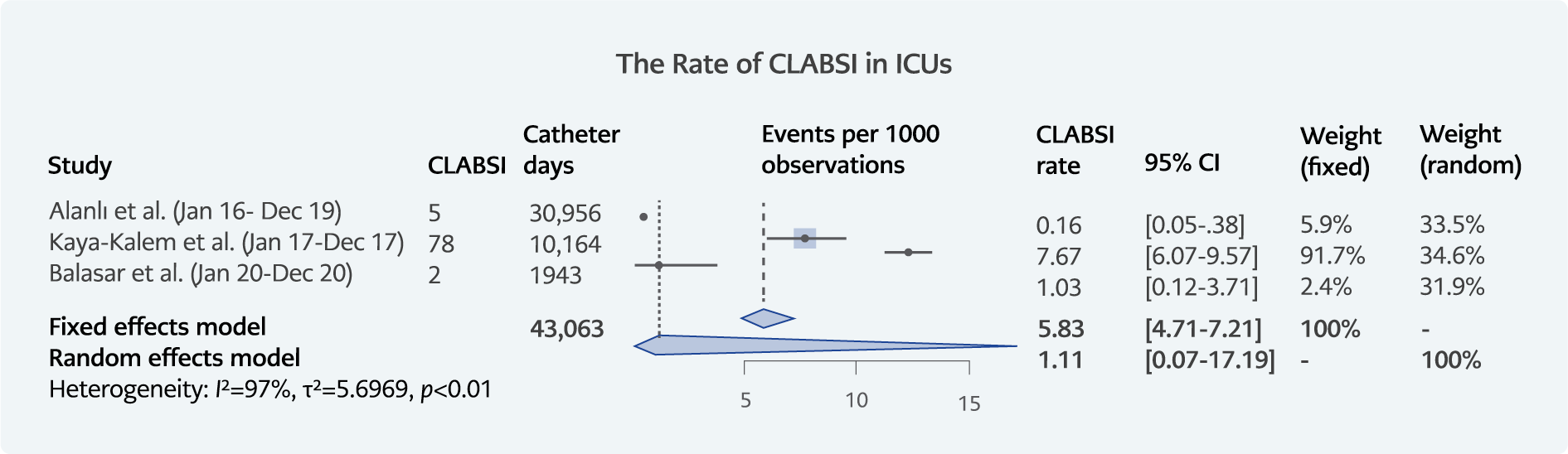
Figure 4. Forest plot of the CLABSI rate from the intensive care unit surveillance.
Surveillance is a key component of any infection control strategy for HAIs and antimicrobial resistance (AMR). With the help of effective surveillance methods of the Republic of Türkiye Ministry of Health, the rate of CLABSI declined from 5.65% to 2.82% (incidence rate ratio [IRR]=0.47, p<0.0001) in 2008 and 2017 in Türkiye (21). In a multicenter study conducted by Azak et al. in 68 hospitals in Türkiye, the CLABSI rate in the adult ICUs was calculated as 7.1/1000 catheter days (22) Atilla et al. reported that the CLABSI rate in the ICUs was 6.20/1000 catheter days (23). In our study, the overall CLABSI rate was calculated as 1.97/1000 catheter days (85/43,063×1000) in ICUs (Figure 4). This rate is lower than the national report and other studies (24). When preparing strategies for infection control measures in healthcare settings, we should aim for zero infection and carry out comprehensive strategies such as campaigns, effective bundle use, brainstorming meetings, and education fairs (23, 25).
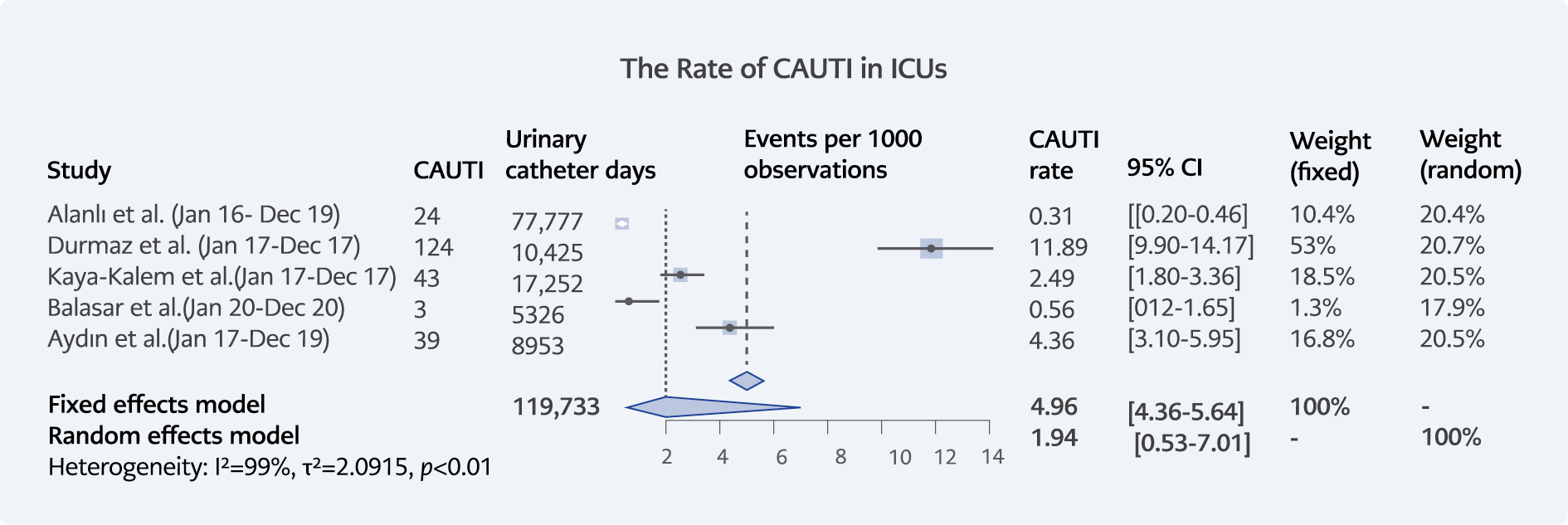
Figure 5. Forest plot of the rate of CAUTI in ICUs in Türkiye.
The rate of CAUTI was calculated as 1.95/1000 catheter days (233/119,733×1000) in ICUs in Türkiye (Figure 5). This rate was announced by the Republic of Türkiye Ministry of Health 2022 Annual Report between 0.4 and 1.7 according to the adult ICU departments (24). The CAUTI rate in the Mix ICU department was 0.7% (24). Therefore, we can comment that the rate of CAUTI can be higher than expected.
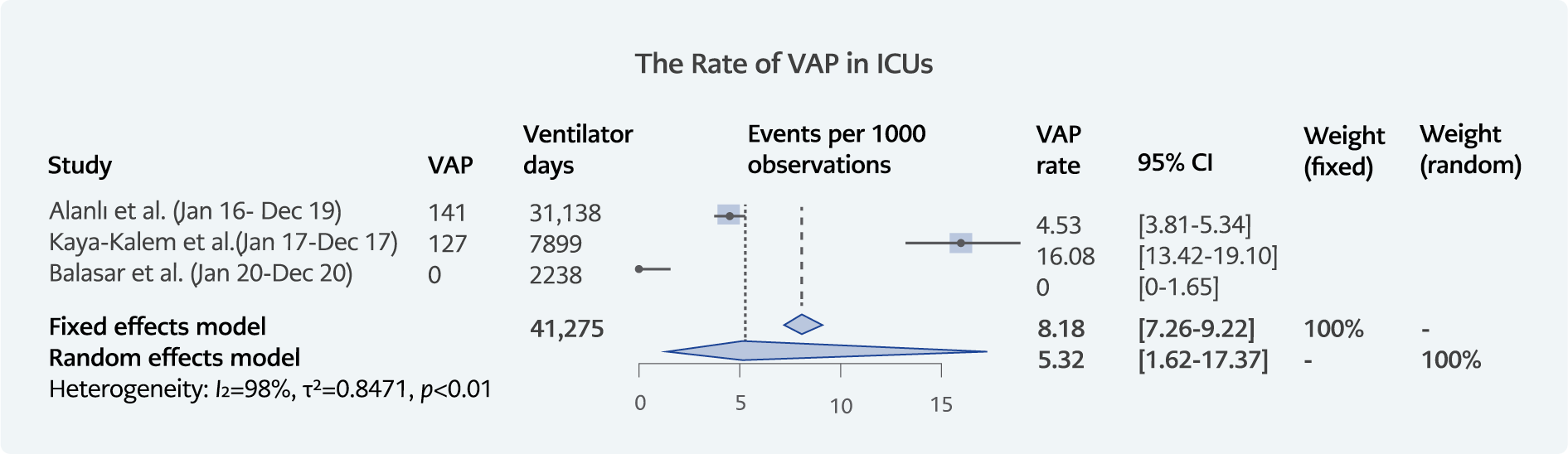
Figure 6. Forest plot of the rate of CAUTI in ICUs in Türkiye.
The last device-associated infection was VAP. We calculated the rate of VAP as 6.49/1000 catheter days (268/41,275×1000) (Figure 6). According to the Ministry’s Annual Report, this rate changed between 0.18 and 10/1000 catheter days in different adult ICU departments in 2022 (24). However, another systematic review included 13 reports from Türkiye by Mumtaz et al. suggested that the rate of VAP could rise to 43/1000 catheter days. Moreover, in their report, the highest mortality rate (66.30%) was reported from a study of Türkiye among 11 countries (26). Despite major advances in microbiological tools and antimicrobial treatment regimens, there is still confusion in VAP’s epidemiology and diagnostic criteria (27). Fernando et al. reported in their study that classical diagnostic criteria such as fever, purulent secretions, hypoxemia, chest radiography, high white blood cell count, positive endotracheal aspirate cultures, or bronchoscopy sampling are not effective in establishing the correct VAP diagnosis. With these criteria, clinicians may misdiagnose VAP cases, and they can order unnecessary antibiotic therapy (28). More studies with higher levels of evidence are needed to evaluate physicians’ diagnostic performance with these definition criteria (29). Improved and simpler methods are urgently needed to facilitate the diagnosis of VAP and promptly initiate effective treatment. Because of these difficulties in diagnosing VAP, the CDC has shifted surveillance from VAP to ventilator-associated event (VAE) surveillance for better comparability and quality improvement (30).
Despite the difficulties in the definition of VAP, healthcare centers should focus on rapid diagnosis and reduce VAP rates with the help of national and international recommendations and guidelines. CDC reported that VAP decreased by approximately 1% in just one year between 2022 and 2021 (from 19% to 18%) (31). The local healthcare centers should be supported by hospital administration and government to get started new interventions according to the needs of centers, such as bundle approaches including head of the bed elevation, peptic ulcer disease prophylaxis, deep venous thrombosis prophylaxis, cuff pressure, subglottic secretion drainage and oral care, education fairs, hand hygiene campaigns.
Surgical site infection (SSI) is the most well-known complication of postoperative procedures, causing psychological and physical problems, prolonging hospital stay, and increasing costs (32, 33). However, the number of comprehensive studies on SSIs in Turkey is limited. For example, in this study, we found no studies conducted in the last 10 years that met the inclusion criteria for the meta-analysis. Healthcare institutions in Turkey are responsible for recording the types of SSIs they find risky in the Republic of Türkiye Ministry of Health system according to their bed capacity. However, institutions are not required to record all the SSIs they detect. This limitation makes it impossible to collect all SSIs and see the extent of the problem. To combat the problem, we must first measure its magnitude accurately. The Ministry should make it mandatory for health institutions to record all types of SSI in the system. In addition, hospitals should be encouraged to plan effective initiatives to improve SSI prevention activities. Infection control committees in hospitals should be authorized to conduct more comprehensive studies on this issue, and their enforcement powers should be increased.
There are several limitations of our study. First, there may be publication bias in the centers as tending not to publish high rates of HAIs. Secondly, a limited number of published surveillance reports covered our inclusion criteria. Third, the quality of published studies was not at the expected level. As researchers, we find it valuable that the studies include commonly identified pathogens that cause HAIs, including resistance rates to some common antimicrobials. Nevertheless, despite the limited number of studies, our meta-analysis includes more than 98 thousand patients from different regions of Türkiye. We can generalize the results of this study, as the rates of each HAI are not much different from the results of the Ministry of Health report.
In conclusion, the rate of HAIs is still high in Türkiye. Surveillance efforts should be encouraged in terms of data collection and dissemination of the outputs. Healthcare settings should focus on zero catheter-associated infections. For this purpose, there is an urgent need for cost-effective control and preventive measures like interventional studies, educational programs on staff training, hand hygiene, awareness of antibiotic resistance, implementation of antibiotic stewardship programs and appropriate use of the bundle approach.