Introduction
COVID-19 is a fatal disease affecting all systems, especially the respiratory system. It manifests with different clinical characteristics, from asymptomatic infection to severe infection (1, 2). Since its initial description, the disease has caused devastating effects and many deaths (3). Predictors of mortality that indicate disease severity play an important role in disease management and treatment decisions (4, 5).
Numerous markers and scoring systems have been studied for COVID-19 as predictors of disease severity and poor prognosis (6-10). The aspartate aminotransferase-to-platelet ratio index (APRI) and the fibrosis-4 (FIB-4) scores are two of these that are readily applicable. APRI and FIB-4 scores are noninvasive markers for predicting the development of liver fibrosis in hepatitis C and nonalcoholic fatty liver disease (NAFLD) (11-13). Novel biomarker-based score (SAD-60), on the other hand, was reported as an indicator of mortality in COVID-19 patients in our previous study (7).
This study aimed to investigate the association between FIB-4 score, APRI, and SAD-60 with mortality in COVID-19 patients hospitalized in a tertiary hospital.
Materials and Methods
Patients at age ≥18 years who were admitted to our hospital for COVID-19 between December 1 and 31, 2021, were included in this single-center retrospective study. Patients with chronic liver disease, malignancies, HIV/AIDS, and pregnant women were excluded. Laboratory diagnosis of COVID-19 was made by SARS-CoV-2 PCR test using nasopharyngeal/oropharyngeal swab specimens. The diagnosis of pneumonia was confirmed by chest CT in patients with the following symptoms: fever, cough, shortness of breath, and tachypnea. Patient demographic, clinical, and laboratory data were retrospectively obtained from patient records. Patient vital signs such as body temperature, peripheral capillary oxygen saturation, respiratory rate per minute at the time of initial admission, and especially blood counts, aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin and D-dimer levels, and other biochemical test results used in the calculation of scores were recorded. The FIB-4 score and APRI were calculated according to the following formulas:
FIB-4 Score= Age (years)×AST (U/L) / [PLT (109/L)×ALT1/2 (U/L)]
APRI= [AST (U/L) / (AST (Upper Limit of Normal) (U/L)] / Platelet Count (109/L)×100
For the SAD-60, the sum of the values of O2 saturation (2.5 points 90%), albumin (2 points < 3.5 g/dL), D-dimer (3.5 points ≥ 0.9µg/ml), and age (2 points ≥ 60 years) were used. Patients were divided into two groups as deceased and survived. A comparative analysis was applied. The predictive ability of the FIB-4 score, APRI, and SAD-60 for in-hospital mortality was evaluated.
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 15.0 (IBM Corp., Armonk, NY, USA). For categorical variables, numbers and percentages were used. The median and interquartile range were used for continuous variables. Rates in groups were compared with the chi-square test. Comparisons of numerical variables between two independent groups were performed with the Student’s t-test for normally distributed data, otherwise with the Mann-Whitney U test. For the prediction of mortality, the FIB-4 score, APRI, and SAD-60 were evaluated by the receiving operating characteristic (ROC) curve. Kaplan-Meier survival analysis was calculated using the breakpoints of the scores. Cox regression analysis was performed to identify risk factors. Results were presented as hazard ratio (HR) and 95% confidence interval (CI). The statistical significance was set as p<0.05.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Haseki Training and Research Hospital on August 24, 2022, with decision number 148-2022. Because this was a retrospective study, patient consent was not obtained.
Results
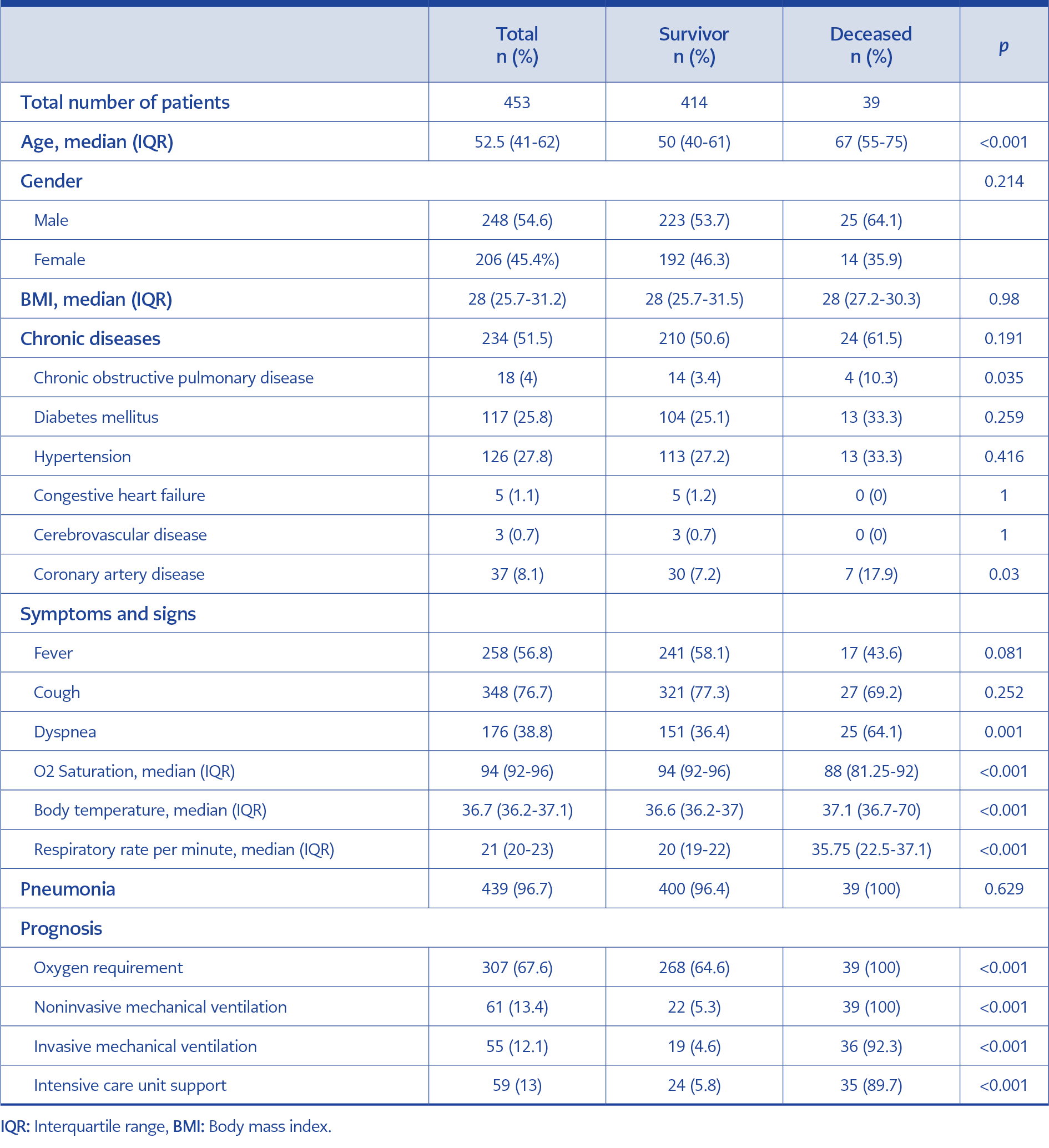
Table 1. Demographic and clinical characteristics of patients diagnosed with COVID-19.
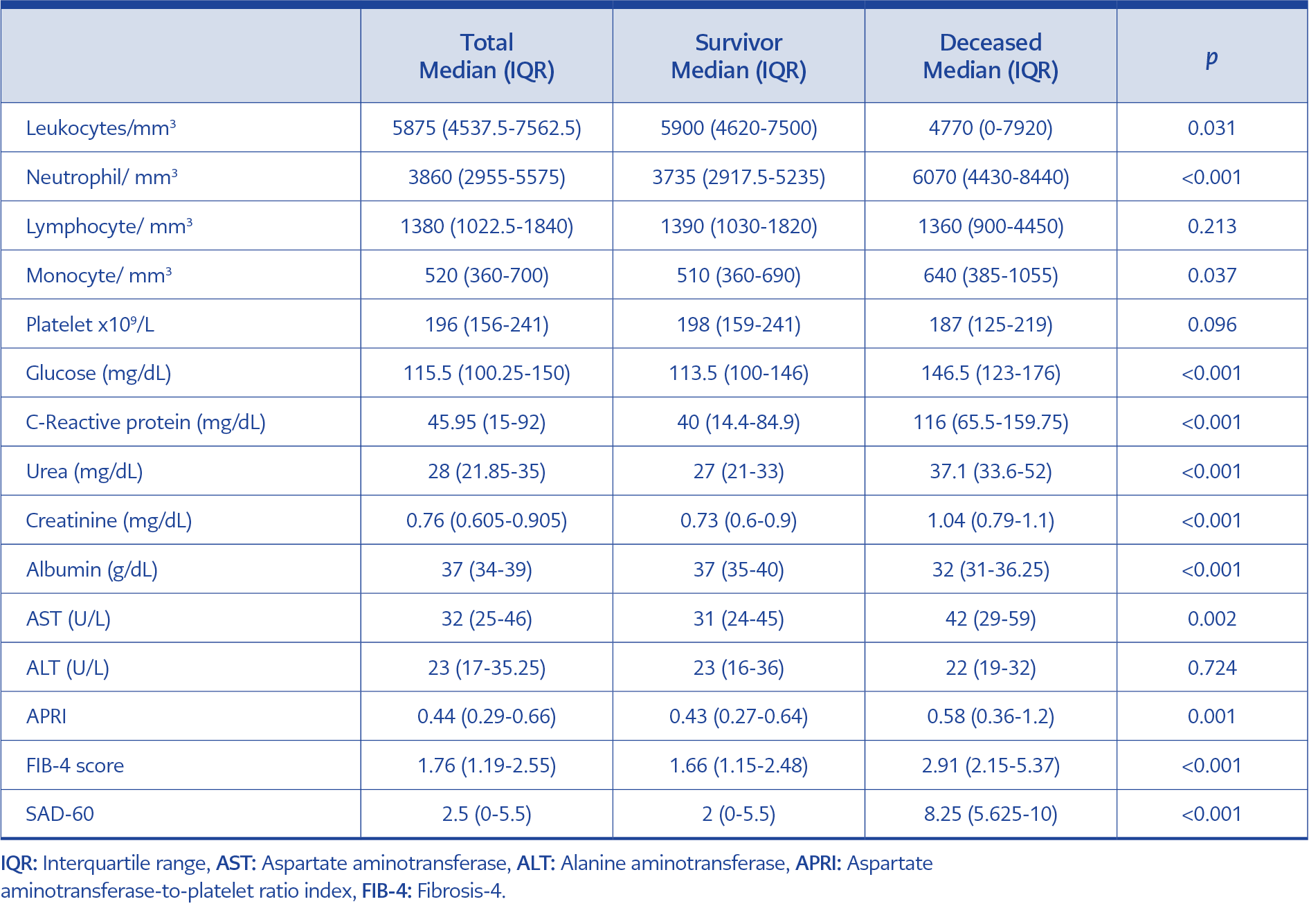
Table 2. Laboratory characteristics of patients diagnosed with COVID-19.
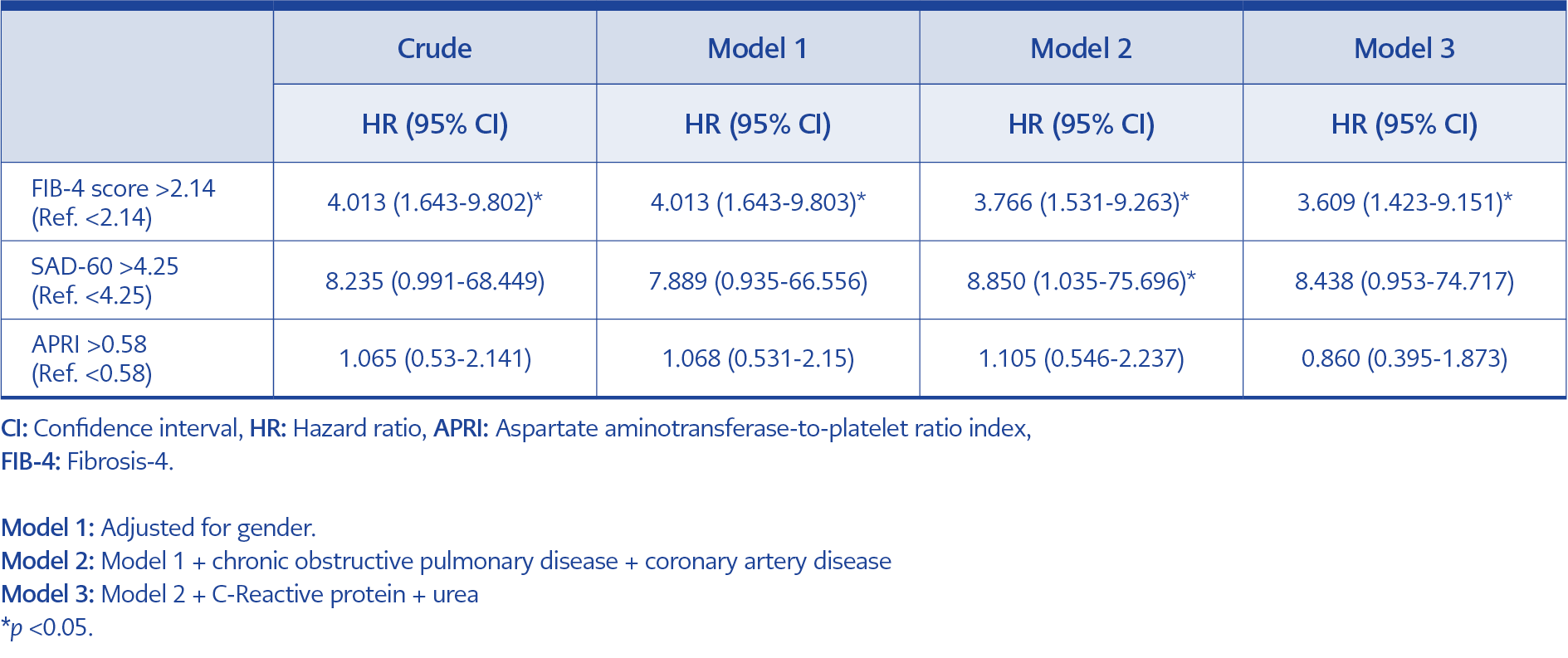
Table 3. Relationships of FIB-4 score, SAD-60, and APRI with mortality.
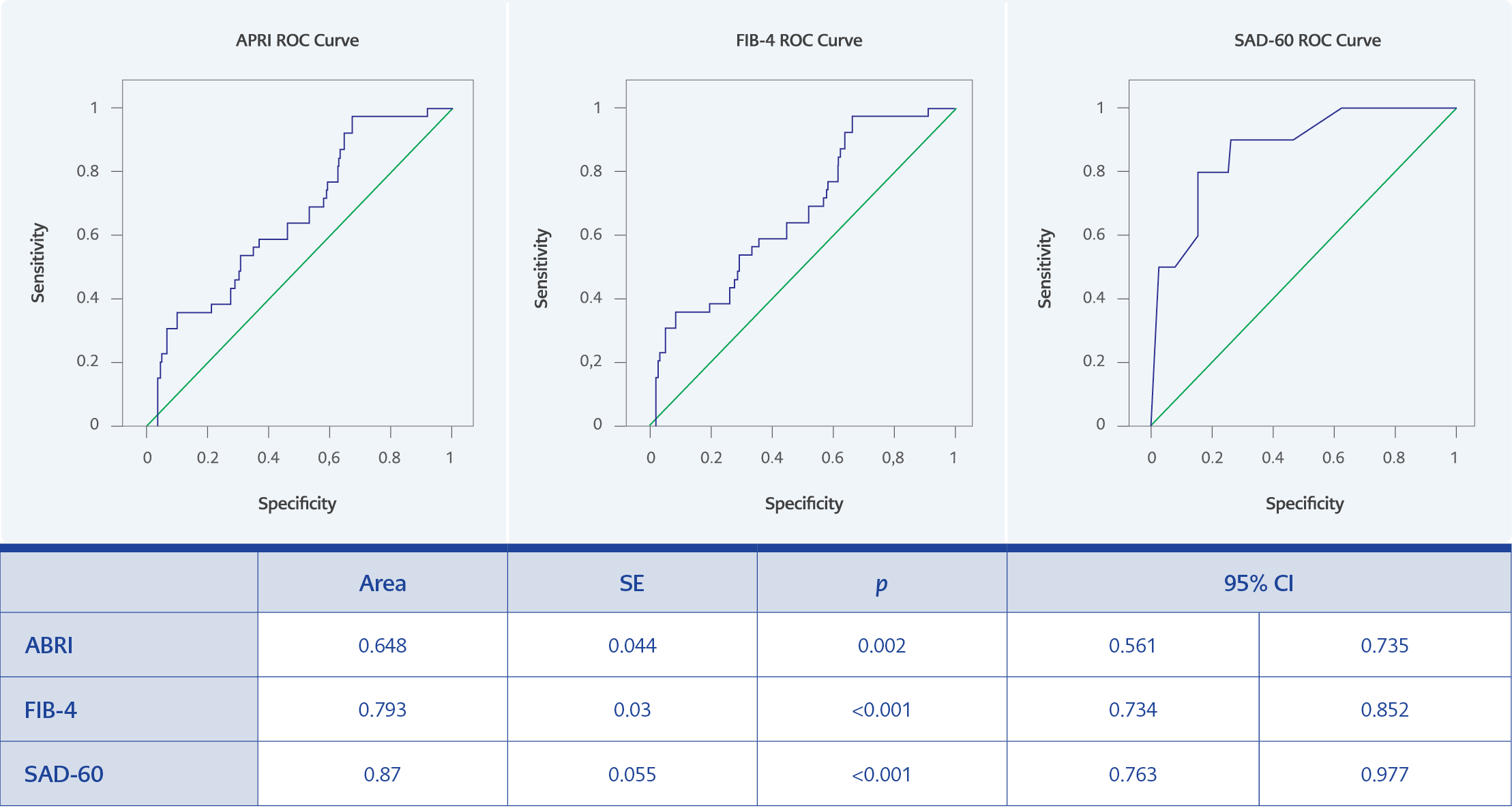
Figure 1. ROC curve analyses of APRI, FIB-4, and SAD-60 scores for predicting mortality in COVID-1.
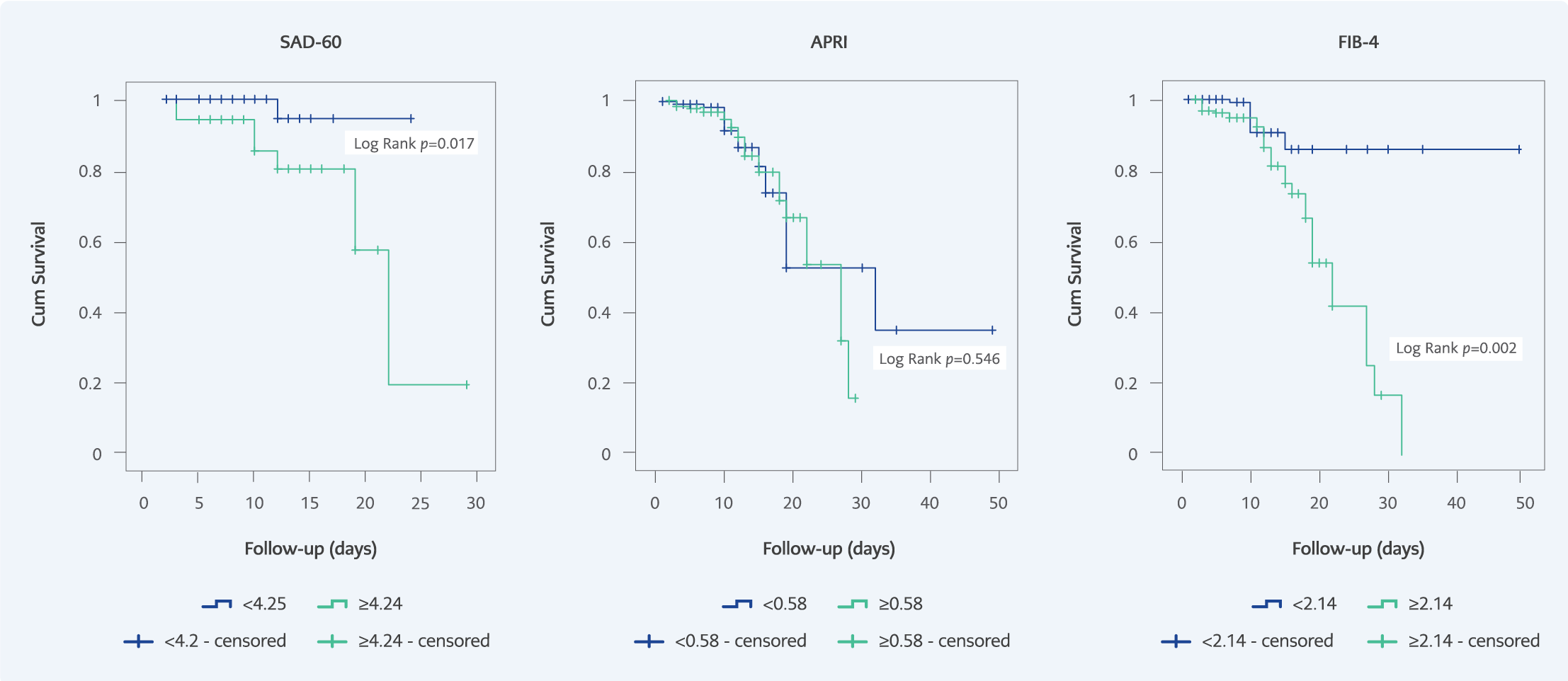
Figure 2. Probability of survival of COVID-19 patients during hospitalization based on APRI, FIB-4, and SAD-60 scores.
Of the 453 patients enrolled in the study, 248 (54.6%) were male and the mean age was 52.5 (41-62) years. Mortality was recorded in 39 (8.5%) of the patients. Causes of death were secondary bacterial pneumonia in 12 (30.8%) patients, multi-organ failure in 10 (25.6%), macrophage activation syndrome in 8 (20.5%), pulmonary embolism in 4 (10.3%), bacteremia in 3 (7.7%), myocardial infarction in 2 (5.1%). The mean age of the deceased group was significantly higher compared with the survivor group (67 years vs. 50 years, p<0.001). The prevalence of chronic obstructive pulmonary disease (COPD) (14 (3.4%) vs. 4 (10.3%); p=0.035) and coronary artery disease (CAD) (30 (7.2%) vs. 7 (17.9%); p=0.030) was higher in the deceased group than in the survived group. In total, 439 had COVID-19 pneumonia and four patients had mild COVID-19 without pneumonia (Table 1). Laboratory results of the patients are shown in Table 2. The scores for APRI (0.43 and 0.58; p=0.001), FIB-4 (1.66 and 2.91, p<0.001), and SAD-60 (2 and 8.25; p<0.001) were higher in deceased patients than in survivors. The optimal cut-off values for predicting mortality in the ROC curve analysis were 0.58 for APRI (sensitivity=56.4%, specificity=63.6%); 2.14 for FIB-4 (sensitivity=79.5%, specificity=68.2%); 4.25 for SAD-60 (sensitivity=90%, specificity=73.8%) (Figure 1). In the Kaplan-Meier survival analysis, the mortality rate in patients with high APRI scores was similar to those with low APRI scores (p=0.546). The mortality rate was higher in patients with high SAD-60 and FIB-4 scores (p=0.017 and p=0.002, respectively) (Figure 2). FIB-4 (HR=4.013, 95% CI=1.643-9.803; p=0.002) and SAD-60 (HR=8.850, 95% CI=1.035-75.696; p=0.046) were found to be independent risk factors for mortality in Cox regression analysis with a model that included gender, COPD, and CAD. APRI (HR=1.105 95% CI=0.546-2.237; p=0.854) was not associated with mortality (Table 3).
Discussion
Our study showed that FIB-4 and SAD-60 scores may be used as predictors of mortality in hospitalized patients with COVID-19. FIB-4 (HR=4.013, 95% CI=1.643-9.803; p=0.002) and SAD-60 (HR=8.850, 95% CI=1.035-75.696; p=0.046) were found to be independent risk factors for mortality in Cox regression analysis.
Although the FIB-4 score is a noninvasive tool primarily used to diagnose liver fibrosis, studies are showing an association between FIB-4 and some chronic diseases and cardiovascular diseases (14-16). Recently, the association between the FIB-4 score and the severity and prognosis of COVID-19 has been the subject of numerous studies (10,17-19). COVID-19 damages not only the lungs but also the liver and other solid organs (20, 21). The impact of liver injury on the prognosis of COVID-19 can be severe, as can that of pneumonia. Although COVID-19 is reported to have more severe consequences in patients with chronic liver disease and a high FIB-4 score, large-scale studies on this topic are needed (22-24). For example, in patients with hepatitis C and SARS-CoV-2 infection, the FIB-4 score was associated with hospitalization but not mortality (6.6% vs. 6.5%; p=0.9) (22). In another study, the FIB-4 score was described as a noninvasive marker for the diagnosis of NAFLD, and an elevated FIB-4 score was also associated with the severity of COVID-19 in these patients (17).
APRI, another score that can be used to determine liver fibrosis, has also been associated with the severity and prognosis of COVID-19. APRI has been frequently compared with FIB-4 in many studies (10, 18, 19, 24, 25). In a study involving 202 hospitalized patients with COVID-19, further analysis that also accounted for gender and liver disease found that each unit increase in FIB-4 was an independent predictor of mortality (odds ratio [OR]=1.79, 95% CI=1.36-2.35; p<0.001). In the same study, APRI did not prove successful in predicting mortality (p=0.054) (10). In another study of COVID-19, containing patients admitted to the emergency department, the FIB-4 score (area under ROC curve [AUC]=0.689, 95% CI=0.659-0.718; p<0.0001) was superior to the APRI in predicting mortality (AUC=0.58, 95% CI=0.553-0.615; p=0.0008). In the same study, FIB-4 was shown to be significantly higher in patients requiring high-flow oxygen and mechanical ventilation, and FIB-4 was also associated with COVID-19 disease severity (18). In a meta-analysis of thirteen studies examining the association between FIB-4 and COVID-19 prognosis, a high FIB-4 score was found to increase mortality 3-fold (OR=3.01, 95% CI=2.21-4.09; p<0.001) (19). Woo-Kim et al. observed 10-fold increased deaths in COVID-19 patients with a high FIB-4 score and diabetes mellitus than in patients with a low FIB-4 score without diabetes mellitus (24). As a result, different cut-off values for FIB-4 and APRI scores were used in mortality studies.
In our study, the presence of any chronic disease (at least one or more) was not associated with mortality, whereas FIB-4 and APRI scores were higher in the deceased group. In the Kaplan-Meier analysis, a higher mortality rate was found in those with FIB-4 score>2.14, but this difference was not found for APRI.
Recent studies have shown that APRI can be used as an early predictor of poor prognosis in COVID-19 patients. However, FIB-4 performs superior to APRI. In a study examining the relationship between liver fibrosis scores and mortality in COVID-19, FIB-4 (C-index=0.74) was found to be superior to APRI (C-index=0.657) (26). In the study of Crisan et al., FIB-4 and APRI scores were found to be significantly higher in the deceased group in patients with COVID-19 (27). The researchers demonstrated that a FIB-4 score of >3.25 increased mortality 1.3-fold (OR=1.353; p=0.046). However, they found that the APRI score was not associated with mortality (OR=0.21; p=0.119) (27). Consistent with the general literature, in our study FIB-4 was superior to APRI in predicting mortality in COVID-19. The predictive value for mortality of FIB-4 (AUC=0.793) and SAD-60 (AUC=0.870) scores seems also to be higher than other previously tested scores for mortality in COVID-19 patients, namely the World Health Organization (WHO) severity scale (AUC=0.654), the national early warning score (NEWS) (AUC=0.649 ), the CURB-65 score (AUC=0.591) and the acute physiological assessment and chronic health evaluation (APACHE) score (AUC=0.651) (28). In our previous multicenter study including 1013 patients, the SAD-60 (AUC=0.776) score was more successful than NEWS (AUC=0.686), CURB-65 (AUC=0.753), and quick sepsis-related organ failure (q-SOFA) (AUC=0.628) scores in predicting mortality in hospitalized patients with COVID-19 (7).
Objective results may not always be obtained with scores that include vital signs. This is because environmental and personal factors may play a role in measuring and recording vital signs in emergency departments and health centers with heavy workloads. Perhaps for this reason, scores obtained with noninterpretable parameters such as laboratory values and age are more successful in predicting disease severity. In our study, the SAD-60 score proved to be superior to FIB-4 and APRI in predicting mortality in hospitalized patients with COVID-19 (AUC=0.870, sensitivity=90%, specificity=73.8%). Further analysis by gender, COPD, and CAD showed that mortality increased about 4-fold in patients with FIB-4 >2.14 and 9-fold in patients with SAD-60 score >4.25.
Since the beginning of the pandemic, advanced age has been known to be associated with increased mortality for COVID-19 (1, 29). Studies evaluating COVID-19 predictors of disease severity have pointed out that age and the presence of chronic disease are important individual factors determining disease severity (30). On the other hand, biochemical tests indicating organ damage and the scores generated from these tests are likely to be successful in predicting disease severity and mortality at COVID-19. The addition of the age factor to the formulas is expected to increase the success of these scores in predicting disease severity. The low success of APRI compared with FIB-4 and SAD-60 may also be due to this reason. Consistent with this, in a multicenter study of 353 patients with COVID-19, the AUC value of APRI (0.66; 95% C= 0.56-0.76) was lower than the AUC value of FIB-4 (0.72; 95% CI= 0.61-0.82) for predicting mortality. However, the APRI-plus AUC value of 0.90 (95%CI= 0.86-0.95), obtained by adding age and other parameters to the APRI, was much more successful than FIB-4 in predicting mortality (25).
This study has several limitations. First, our results may not be generalizable because the study was conducted in a single center. Second, the scores were calculated based on biochemical parameters at the time of initial admission. Therefore, a longitudinal evaluation was not performed. Third, NAFLD patients could not be excluded because routine abdominal ultrasonography was not performed in COVID-19 patients. Nevertheless, this study has some strengths. First, several variables, such as demographic features, clinical characteristics, and laboratory test results, were included in the study, and multivariable analyses were performed. Second, our study population was homogenous including only COVID-19 patients confirmed by the nasopharyngeal/oropharyngeal SARS-CoV-2 PCR testing.
In conclusion, the performance of SAD-60 and FIB-4 scores, composed of age and biochemical parameters, seems to be better than that of scores containing vital signs in predicting a poor prognosis for COVID-19. Therefore, SAD-60 and FIB-4 scores are easily applicable and may be used to predict mortality in COVID-19 patients.