Introduction
Fascioliasis is a neglected tropical disease caused by liver flukes, Fasciola hepatica or Fasciola gigantica, and affects at least 2.4 million people worldwide, according to World Health Organization (WHO) estimates (1). Sheep and cattle are the natural definitive hosts of F. hepatica infection; therefore, fascioliasis is common in sheep-raising regions where freshwater plants are consumed.
The frequency of fascioliasis is low even in infectious disease clinics, and clinical presentation with liver abscess but without eosinophilia is unexpected. We present a 57-year-old female patient by focusing on challenges in diagnosis and treatment.
Case Presentation
A 57-year-old female was admitted with fever, nausea, vomiting, loss of appetite, and weight loss within the last two months. She had diabetes mellitus (DM), hypertension, hyperlipidemia, and mitral valve insufficiency. Her surgical history included cholecystectomy, thyroidectomy, percutaneous transluminal coronary angioplasty, and obesity surgery. The patient’s father had stomach cancer and DM, and her mother was diagnosed with DM and myocardial infarction.
On admission, body temperature was 38.6 ºC, blood pressure 110/70 mmHg, pulse 78 beats per minute, and respiratory rate 18 per minute. The patient had tenderness on the right side of the abdomen. Before hospital admission, 16 mg of candesartan and 12.5 mg of hydrochlorothiazide were administered to control blood pressure. In addition, 1000 mg metformin and 50 mg vildagliptin were prescribed twice daily.
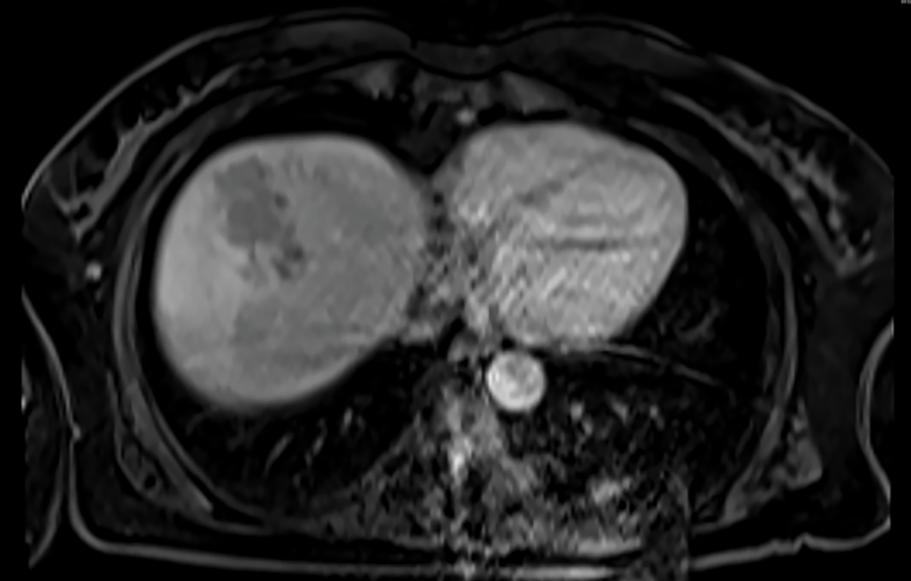
Figure 1. The axial MRI images of encapsulated Fasciola hepatica burrows.
Leukocytes 11,300/µL, hemoglobin 8.3g/dL, CRP (C-reactive protein) 80 mg/L (normal range=0-5), procalcitonin 0.03 ng/mL, creatinine 0.7mg/dL were detected. In abdominal magnetic resonance imaging (MRI), there was a 7 cm x 5.5 cm contrast-enhancing mass consisting of multiloculated solid and cystic components (Figure 1). Ultrasonography-guided drainage was performed with suspicion of liver abscess. Abscess and blood samples were obtained for microbiological analysis. Ceftriaxone 2 g every 24 hours and metronidazole 500 mg every 6 hours were started. There was no growth in the cultures. Her fever subsided, her CRP level decreased to 30 mg/L, and she was discharged with oral antibiotics.
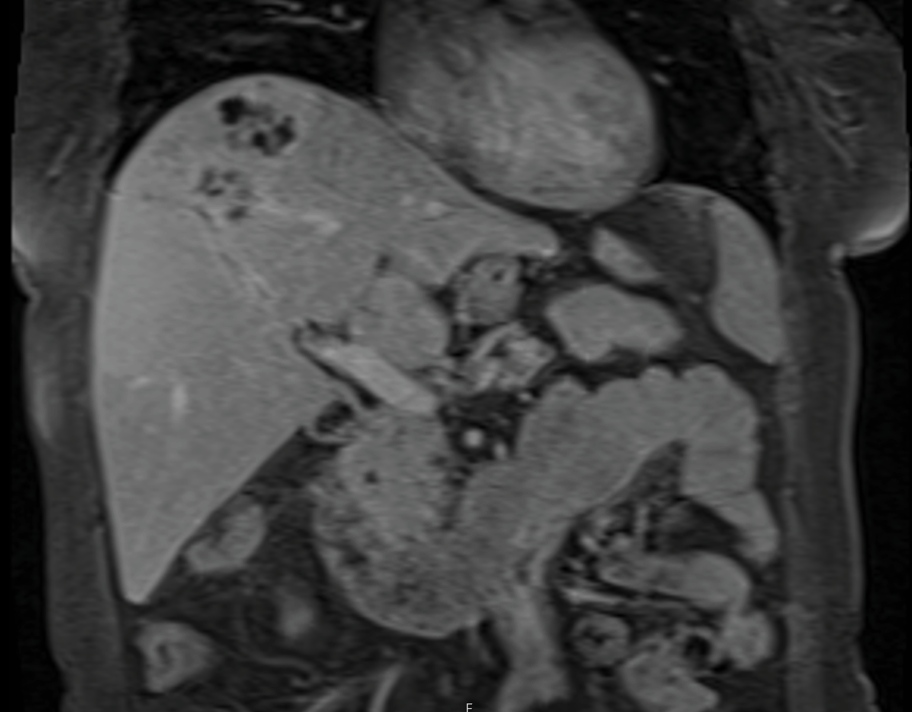
Figure 2. MRI images with contrast, T1 series.
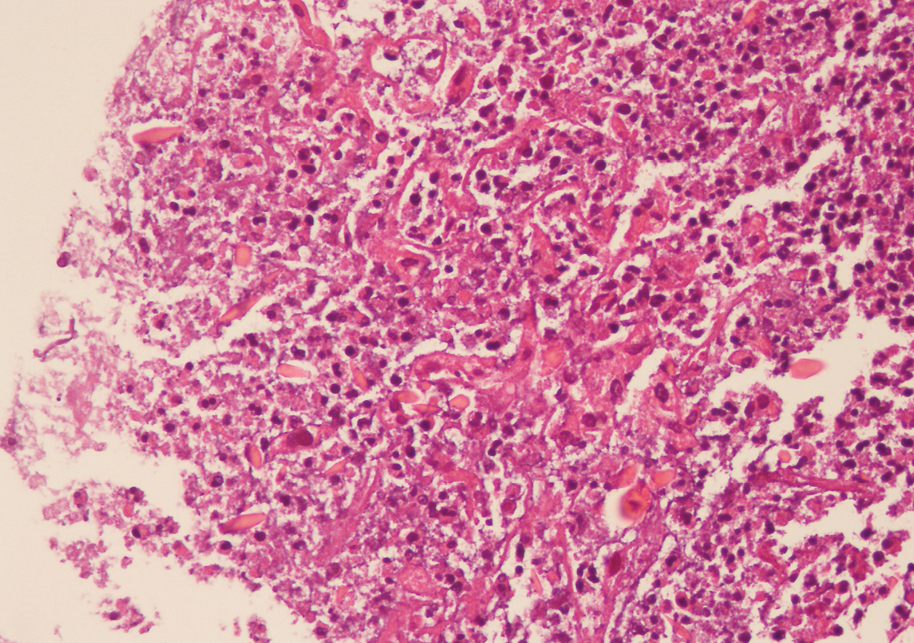
Figure 3. Histopathology showing inflammation and parasitic infection, hematoxylin, and eosin stain.
On the 20th day of antibiotics, she had a fever again, and no improvement was observed in the abdominal MRI. Treatment was switched to 1 g daily ertapenem for three weeks. The MRI was repeated during the third week of antibiotics, and a biopsy was performed due to the enlargement of the abscess (Figure 2). Fever, itching, anemia, acute renal failure, hyperbilirubinemia, and eosinophilia were detected following the biopsy; however, she improved within the next few days of her intensive care unit (ICU) admission. The histopathology for aspiration biopsy of the abscess revealed inflammation and parasitic infection (Figure 3). A history of raw meat and freshwater plant consumption was discovered upon questioning.
Cryptosporidium parvum, Entamoeba histolytica, and Giardia lamblia were investigated in stool via conventional microscopy and cassette tests (Crypto-Giardia-Entamoeba MonlabTest®; Monlab: Services for Clinic Diagnostic Laboratories, Barcelona, Spain) for antigens but results were negative. Two weeks later, F. hepatica antibodies tested positive in an outside laboratory via enzyme-linked immunosorbent assay (ELISA). Triclabendazole was not readily available, but it was obtained abroad and given 2×10 mg/kg for one day. Similar cases among the patient’s family and friends were inquired about, revealing fascioliasis in her friend one year ago. Fever, itching, and eosinophilia declined after using triclabendazole. MRI was repeated in the first, sixth, and twelfth months of triclabendazole, and regression was observed.
Discussion
Even though fascioliasis is a worldwide disease, its impact can be devastating for high-prevalence countries (2). The prevalence of F. hepatica was found to be 0.1% among positive stool samples in İstanbul between 1999 and 2009 (3); however, the seroprevalence of fascioliasis was higher and found to be 5.5% according to a recent report (4). Another study reported a cluster including 24 cases from the same family (5). The complications of the infection increase the economic burden of fascioliasis at both individual and government levels. Nevertheless, inequalities in disease burden require better diagnostic tools, and widely available treatment options are needed.
F. hepatica enters the gastrointestinal tract by the ingestion of contaminated freshwater plants or contaminated water and travels to the liver. The burrows of the parasite can be visualized in MRI images (6), as illustrated in Figure 1-2. The infection in the liver starts with an acute phase accompanied by eosinophilia (7), fever, and pain. During this hepatic phase of the infection, liver enzymes (8) increase dramatically. However, the presented patient had no eosinophilia because eosinophilia and acute phase reactant response subsides after the immunologic response. Instead, it is replaced with low-grade inflammation that explains the presenting symptoms of persisting fever, loss of appetite, and weight loss.
Enzyme-linked immunosorbent assay (ELISA) is the preferred diagnostic test for F. hepatica antibodies in the sera (8). However, the western blotting technique (9, 10), polymerase chain reaction-restriction length polymorphism (PCR-RFLP) method (11), and loop-mediated isothermal amplification (LAMP) (12) assay are also available. Although serology testing has been known for its high sensitivity and specificity, the unequal distribution of disease incidence poses a real challenge for diagnostic tool design. In our case, ELISA was used for F. hepatica antibodies because of its availability and reliability in the clinical setting.
Following the diagnosis of fascioliasis, treatment with the proper anti-parasitic agent might shorten the duration of hospitalization and increase recovery speed (13). Triclabendazole is the treatment of choice in F. hepatica infection, although this anti-helminthic drug is not available in many countries such as Turkey, and it should be obtained abroad, delaying treatment. Although surgical interventions are anecdotal (14), second-line antibiotics are lacking. Praziquantel in trematode infections (15) is another treatment approach, yet resistance can emerge. Fortunately, the case discussed in this article had a triclabendazole-susceptible strain; nevertheless, the genomic testing of the parasite was not performed, and susceptibility was deducted from the clinical response.
In conclusion, it should be considered that F. hepatica might be responsible for liver abscesses in an endemic region when antibiotic treatment fails. The diagnosis relies on serological testing of F. hepatica antibodies in the sera. Although triclabendazole is the first line of therapy for fascioliasis, it is not available in many countries and should be obtained abroad, causing delays in treatment.