Introduction
Hepatitis B virus (HBV) infection remains a significant public health issue globally. According to the latest data released by the World Health Organization (WHO) in July 2023, the number of individuals living with chronic hepatitis B (CHB) infection as of 2019 was reported as 296 million, with 820 million deaths attributed to cirrhosis and hepatocellular carcinoma (HCC) resulting from HBV infection (1).
CHB patients positive for hepatitis B e antigen (HBeAg) constitute a group of patients critical regarding fibrosis or hepatocarcinogenesis (1). According to the European Association for the Study of the Liver (EASL) 2017 guidelines, in HBeAg-positive chronic infection, very high HBV DNA and normal alanine aminotransferase (ALT) levels with minimal or no necroinflammation and fibrosis in the liver are observed. However, it is noted that hepatocarcinogenesis continues. In CHB with HBeAg positivity, patients’ liver enzymes are high and characterized by moderate-severe necroinflammation and fibrosis. Although there is an association between HBV DNA levels and higher risk of cirrhosis and HCC in CHB, the severity of liver fibrosis is not consistently associated with HBeAg-positive disease.
According to the EASL guidelines, antiviral therapy is recommended for HBeAg-positive chronic infection in individuals over 30 years of age and HBeAg-positive CHB patients regardless of age without the requirement of biopsy, while in Türkiye, antiviral treatment cannot be initiated in hepatitis B patients without liver biopsy, and fibrosis demonstrated in the biopsy according to the Health Implementation Communiqué criteria (2). Therefore, in the course of HBeAg-positive patients, sensitive and specific non-invasive evaluations should be performed to detect the progression of the disease early, which will also prevent unnecessary biopsies (3, 4). This study aimed to determine predictors of advanced fibrosis score and HAI in HBeAg-positive patients who underwent liver biopsy.
Materials and Methods
Between January 2015 and December 2022, treatment-naïve patients with HBeAg-positive CHB infection aged 18 years or older were included in the study. HBeAg-negative patients and patients with unavailable HBeAg records were excluded. Among HBeAg-positive patients, patients with significant alcohol consumption, malignancy cases, hepatitis C virus (HCV) coinfections, patients with previous antiviral treatment for CHB, and patients with insufficient data were excluded. Eventually, patients with HBeAg-positive CHB who underwent liver biopsy were included in the study.
Demographic data (age, gender), laboratory findings (ALT, AST, platelet [PLT] count, albumin, total bilirubin, fasting blood sugar, alpha-fetoprotein [AFP], international normalized ratio [INR], HBV DNA), and liver biopsy results were retrospectively recorded from the hospital electronic system. Ishak score and histological activity index (HAI) were used to assess fibrosis and necroinflammation (5). For each patient, the “AST to platelet ratio index” (APRI) and fibrosis-4 (FIB-4) scores were calculated. The APRI score was calculated as APRI=AST/AST upper limit × 100/PLT (109 /L), while the FIB-4 score was calculated as FIB-4=Age (years) × AST (U/L) / ALT (U/L) × PLT (109 /L) (6). Ultrasound examination of patients was evaluated for liver size, irregularity, and mass lesions. In the study, patients with HAI ≥6 and/or fibrosis ≥2 were considered to have significant liver damage.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 15.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were given as numbers (n) and percentages (%) for categorical variables and median with interquartile range for continuous variables. Categorical variables were compared using the chi-square test. Independent two-group comparisons of continuous variables were performed using the Mann-Whitney U test, as the numerical variables did not meet the conditions for normal distribution. Cut-off values for albumin were determined by receiver operating characteristics (ROC) curve analysis. Independent determinants were identified by univariate and multivariate logistic regression analysis. The statistical significance was set as p <0.05.
Results
During the study period, there were a total of 731 patients who tested positive for HBsAg. After excluding 598 HBeAg-negative patients and 52 patients with unavailable HBeAg records, 81 HBeAg-positive patients were identified. Among them, four individuals with significant alcohol consumption, two malignancy cases, two hepatitis C virus coinfections, four patients with previous antiviral treatment for HBV, and three patients with insufficient data were excluded. Eventually, 66 patients were included in the study; 34 (51.5%) were male, and the median age was 26 (22.7-34.2) years.
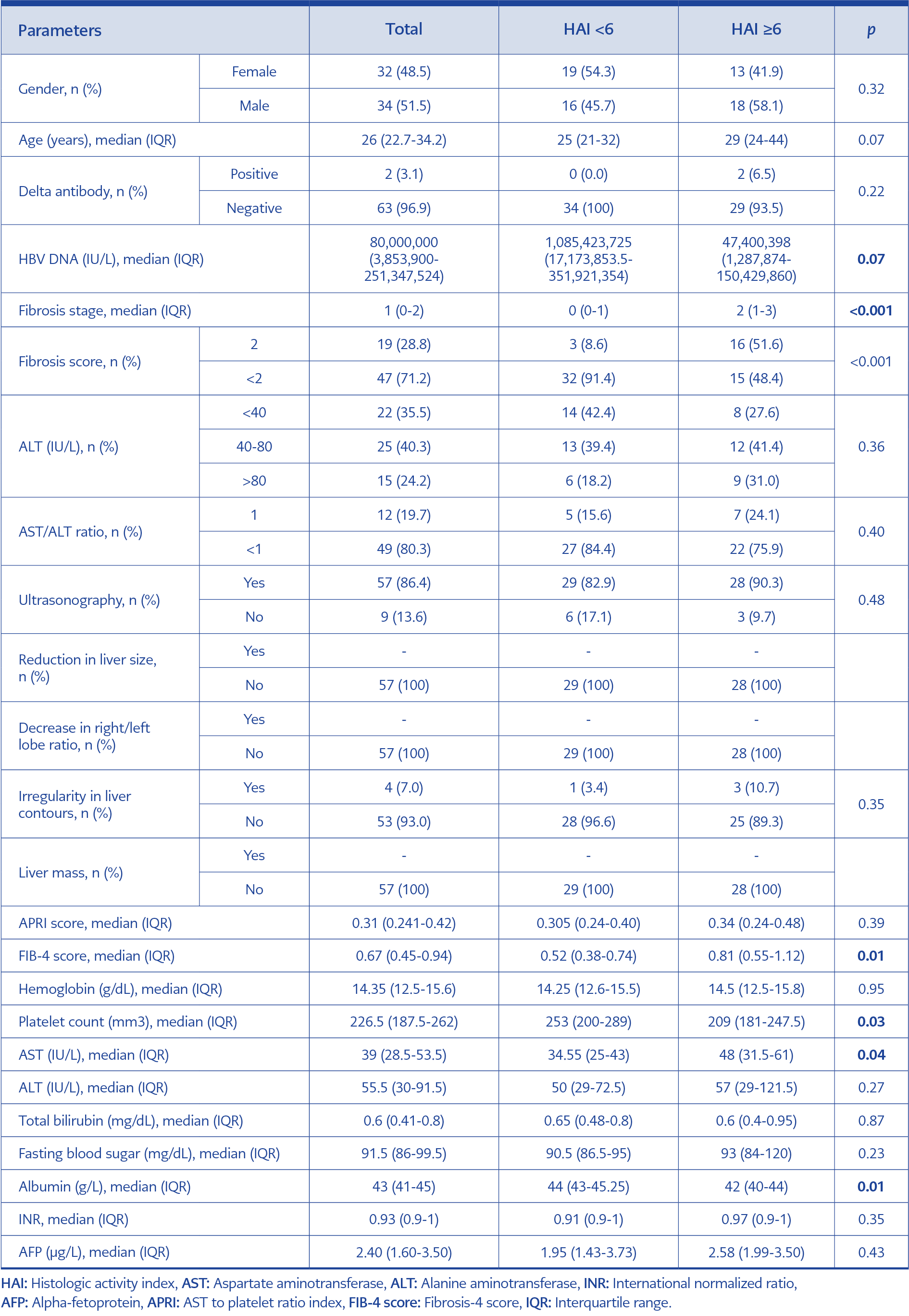
Table 1. Comparison of laboratory and radiological findings of patients with HAI ≥6 and HAI <6.
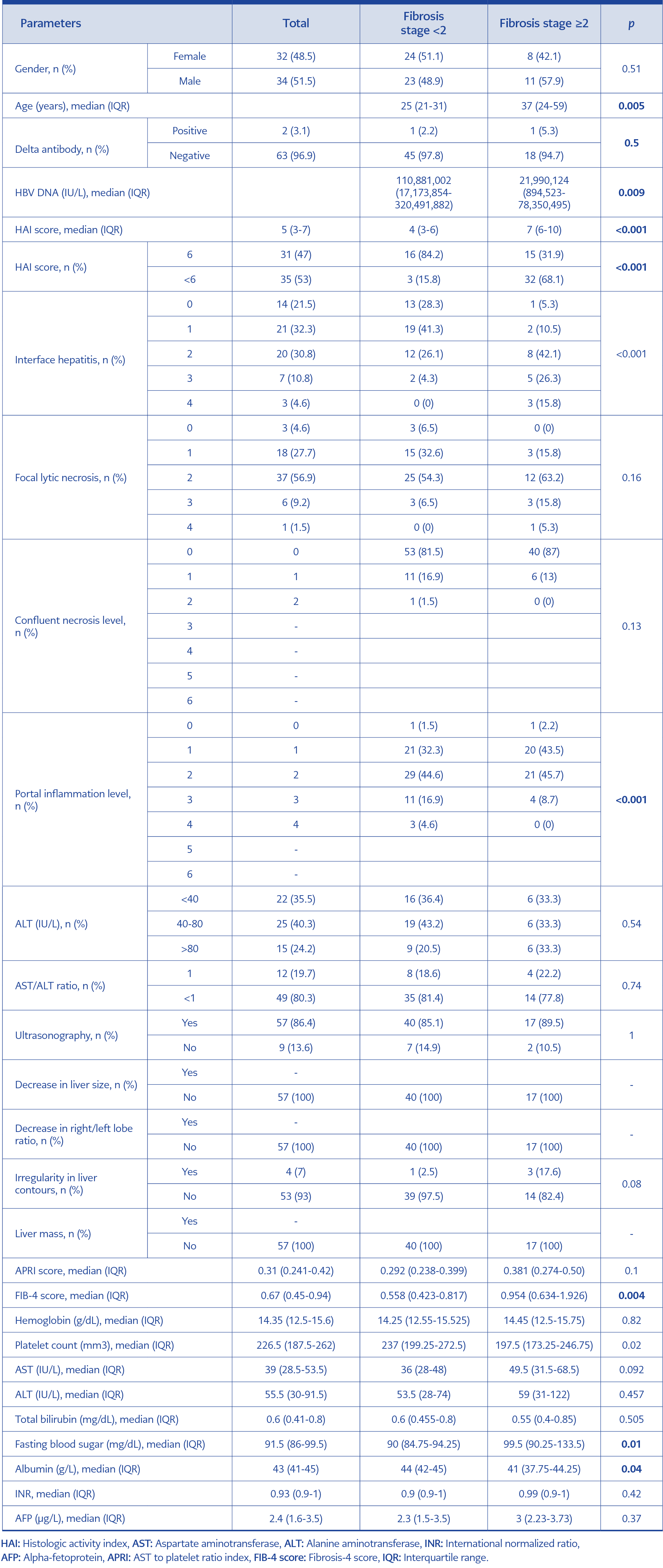
Table 2. Comparison of laboratory and radiological findings of patients with fibrosis ≥2 and fibrosis <2.
In the evaluation of necroinflammation, age (p=0.07) and gender (p=0.32) did not significantly differ between HAI <6 and HAI 6. While ALT level (p=0.36) and AST/ALT ratio (p=0.40) did not significantly differ for HAI, AST level was significantly higher in patients with HAI ≥6 than in patients with HAI <6 (p=0.04). Albumin level (p=0.01) and PLT count (p=0.03) were lower in patients with HAI 6, while the FIB-4 score was found to be significantly higher (0.01) (Table 1). In the assessment of fibrosis, there was no significant difference in gender among patients with FIB-4 ≥2 (p=0.51). However, compared to those with FIB-4 <2, age was significantly higher in patients with fibrosis grade ≥2 (37 years vs. 25 years, p=0.005). The HAI score (p<0.001), HAI ≥6 ratio (p<0.001), and FIB-4 score (p=0.004) were significantly higher in patients with FIB ≥2 compared to those with FIB-4 <2. The HBV DNA level in patients with FIB-4 ≥2 was lower than in patients with FIB <2 (p=0.009). Additionally, the FIB-4 score (p=0.004) and fasting blood sugar (p=0.01) were significantly higher in patients with FIB-4 ≥2, while platelet count (p=0.02) and albumin levels (p=0.04) were lower in patients with compared to those with FIB-4 <2 (Table 2).
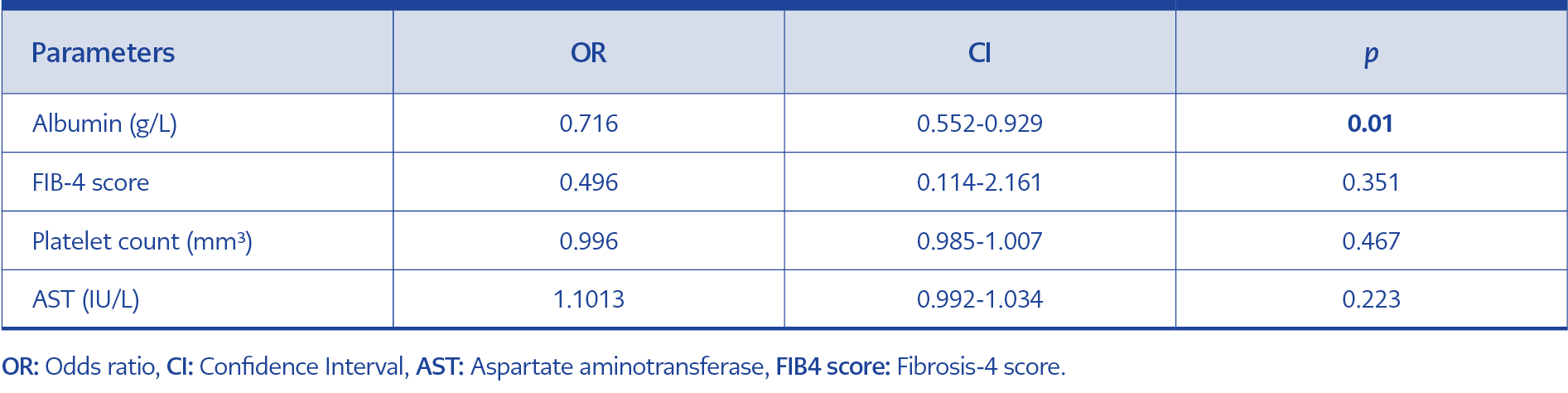
Table 3. Multivariable logistic regression analysis for HAI ≥6.
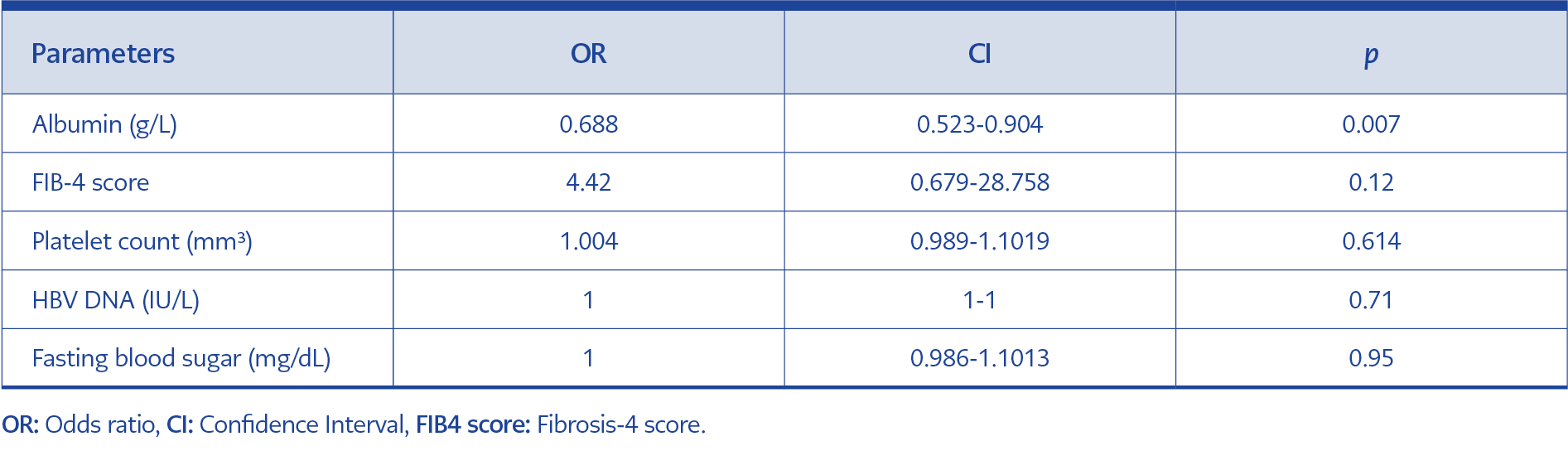
Table 4. Multivariable logistic regression analysis for fibrosis ≥2.
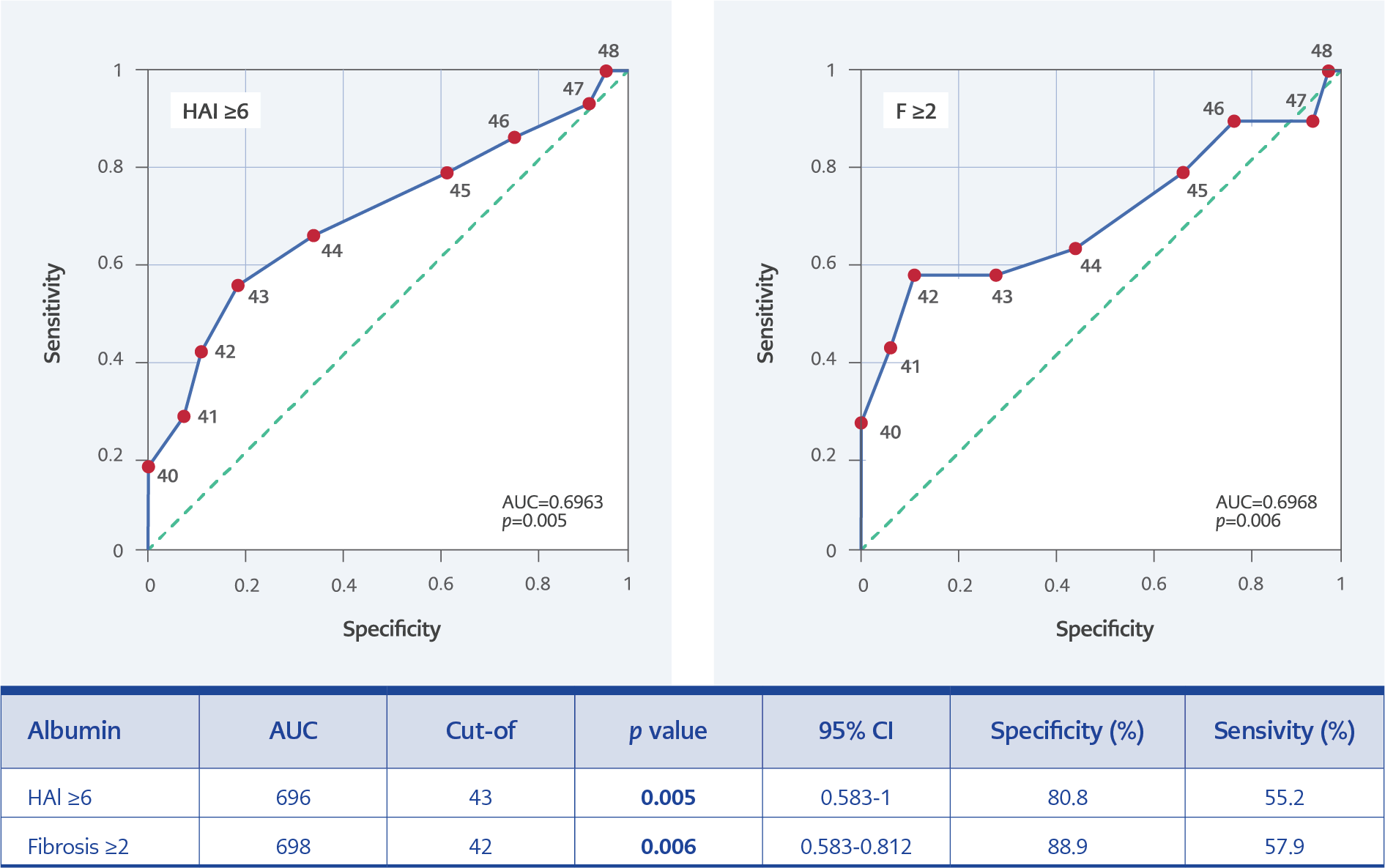
Figure 1. The ROC analysis for albumin in HAl ≥6 and fibrosis ≥2.
Multivariate logistic regression analysis revealed that albumin was the only predictor for HAI ≥6 (p=0.012) (Table 3). In the multivariate analysis model including albumin, FIB-4 score, HBV DNA, PLT count, and fasting blood sugar, albumin level was found to be a predictor for fibrosis ≥2 (p=0.007, odds ratio [OR]=0.688, 95% confidence interval [CI]=0.523-0.904) (Table 4). According to the ROC curve, for predicting HAI≥6 area under ROC (AUROC), values of albumin were 0.696 (sensitivity=55.2%, specificity=80.8%; p=0.005) and for predicting fibrosis ≥2 AUROC values of albumin were 0.698 (sensitivity=57.9%, specificity=88.9%, p=0.006) (Figure 1).
Discussion
This study addresses an important knowledge gap concerning predictors of liver fibrosis and histological activity in patients with HBeAg-positive CHB undergoing liver biopsy. HBV infection remains a significant global health issue, with millions of individuals living with chronic infection and substantial morbidity and mortality associated with cirrhosis and HCC resulting from HBV infection (1). Despite the availability of guidelines for managing HBV infection, there are variations in practice across different regions, highlighting the need for studies like this to provide insights into specific patient populations (3).
One of the key findings of this study is the identification of albumin as an independent predictor of liver damage in HBeAg-positive CHB patients in the multivariate logistic regression analysis. This finding underscores the importance of serum albumin levels as a biomarker for assessing liver function and disease severity in these patients. The study also highlights the significance of other parameters such as age, AST level, PLT count, and FIB-4 score in predicting liver damage, consistent with findings from previous research.
HBeAg positivity is a significant indicator of liver damage, and viral replication. The correlation between high HBeAg levels and high HBV DNA levels has been shown in various studies (7). High HBV DNA levels have also been associated with liver damage and fibrosis (8). Although high DNA levels are demonstrated in HBeAg-positive patients, their relationship with liver fibrosis is not consistent. This inconsistency may lead to delayed detection of liver damage and progression of fibrosis (9). We found no correlation between HBV DNA levels and histological activity. Additionally, in patients with fibrosis grade ≥2, HBV DNA levels were significantly lower compared to those with fibrosis grade <2. The lack of a consistent association between HBV DNA levels and liver fibrosis in HBeAg-positive patients (<35 years of age) observed in this study is notable. This finding suggests that HBV DNA levels alone may not be sufficient for predicting liver damage and underscores the importance of incorporating multiple parameters into disease assessment.
In a study by Liu et al., it was observed that HBV DNA levels were higher in patients with advanced fibrosis compared to those with mild fibrosis in the HBeAg-positive patients (10). When considering the data in the literature and our findings, it is thought that HBV DNA alone is not sufficient for predicting liver damage. In a study with 181 HBeAg-positive patients, age, ALT level, and albumin level were identified as independent predictors for histological liver damage (11). Another study that included HBeAg-positive patients also found a relationship between advanced age and fibrosis (12). Although age was significantly higher in patients with fibrosis ≥2 in our study, we did not find a relationship in multivariate analyses. Çeviker et al. showed in their study that HBeAg or AntiHBe positivity did not affect fibrosis (8). In our previous study, the rate of patients with fibrosis grade ≥2 was found to be 24.5% in HBeAg-negative patients (13). In our study with HBeAg-positive patients, the rate of fibrosis grade ≥2 was 28.8%, which was similar to that of HBeAg-negative patients. In the study by Diktas et al. with 214 patients, a positive relationship between fibrosis and ALT was shown in the HBeAg-positive group (14). Also, another study found a relationship between ALT levels and liver damage (15). In our study, although the ALT levels of the patients in the group with liver damage were higher, this elevation was not statistically significant.
Gao et al. showed in their study that AST, platelet count, and albumin level were independent predictors of liver damage (16). In another study, it was emphasized that AST and age could help predict liver inflammation in HBeAg-positive CHB patients with ALT levels ≤2x upper limit of normal (ULN) (17). In our study, platelet count was significantly associated with both fibrosis score and HAI, while AST level was associated only for HAI. However, these two parameters were not significant in multivariate analysis. Of the patients in our study, 24.2% had ALT levels >2x ULN.
In our study, a high FIB-4 score was found to be significant for both HAI ≥6 and fibrosis ≥2, and in different studies including HBeAg-positive patients, the FIB-4 score was shown as a predictor of liver damage (18, 19). In another study with 520 patients, the effectiveness of FIB-4 and APRI scores was compared with fibroscan, and the performance of FIB-4 scores was almost similar to APRI (20). APRI and FIB-4 were found to be correlated with the severity of fibrosis in liver biopsies, and non-invasive tests used to detect liver fibrosis in individuals with CHB. However, these indices do not eliminate the need for liver biopsy, but can give an idea about the fibrosis status of patients (21).
Studies showed a negative correlation between platelet count and fibrosis (22, 23). In our findings, platelet count was lower in patients with high HAI and fibrosis score, consistent with the literature. There are different studies showing that low albumin levels are determinants in predicting liver damage (16, 17). In the study by Kawaguchi et al. with 155 patients, it was found that the value of albumin was lower in the group developing complications related to advanced fibrosis and cirrhosis in non-alcoholic steatohepatitis patients compared to those who did not develop (11). In another study, suppressing viral replication with lamivudine in CHB patients improved hepatic synthesis function and provided an annual increase of 1.85 g/L in serum albumin level (24). In the multivariate logistic regression analysis conducted in our study, albumin was found as an independent predictor for both HAI ≥6 and FIB-4 ≥2.
There are some limitations to our study. First, it was conducted retrospectively in a single center. Second, biopsy specimens were evaluated by different pathology experts. Additionally, since HBeAg-negative patients were not included in the study, the sample size may be considered relatively small. However, it was vital to evaluate only HBeAg-positive patients to achieve homogeneous results specific to this group.
In conclusion, albumin was found to be an independent predictor of liver damage in HBeAg-positive CHB patients. The fact that the optimal threshold values detected for both HAI ≥6 and fibrosis ≥2 in this patient group were close to normal values suggests that clinicians should be more cautious in monitoring albumin levels and other pre-defined parameters to avoid delays in diagnosis.