Introduction
Cytomegalovirus (CMV) is a DNA virus from the Herpesviridae family that can remain latent in the body for life after primary infection and reactivate and cause viral shedding, especially in cases of immunosuppression (1). In studies conducted in different patient groups from Türkiye, CMV seroprevalence was reported to be between 85-100% (2-4). CMV can affect any part of the gastrointestinal tract, from the oral cavity to the rectum, but it most commonly affects the colon. Colon involvement is reported most frequently. CMV colitis may present with symptoms such as diarrhea, rectal bleeding, abdominal pain, fatigue, and fever and is extremely rare in immunocompetent patients. Immune dysfunction observed in inflammatory bowel disease (IBD) and immunosuppressive treatments facilitate CMV reactivation (5). It is tough to distinguish IBD exacerbation from CMV colitis because they have similar clinical presentations (6).
Isolation of the virus or detection of viral proteins (antigens) or nucleic acid in any tissue sample without symptoms or findings is defined as CMV infection (7). Detection of CMV DNA in blood/plasma is referred to as CMV DNAemia (8). CMV gastroenteritis/colitis is an inflammatory condition that occurs in the intestinal mucosa due to CMV infection (9). The most commonly used pathological and molecular methods for diagnosing CMV colitis include routine hematoxylin and eosin (H&E) staining, immunohistochemistry (IHC), and tissue polymerase chain reaction (PCR). Owl-eye-shaped cytomegalic cells with viral inclusion bodies on H&E staining indicate a CMV infection. While the specificity of H&E staining is high (92%-100%), its sensitivity varies and is relatively low (10%-87%). Currently, IHC is considered the gold standard method for identifying CMV in tissue sections (10). The diagnostic sensitivity can be increased by identifying CMV early antigen using monoclonal antibodies with IHC staining (11). CMV DNA can be detected in colon tissue using the tissue PCR method. However, it is important to correlate this with other histological findings to associate it with latent CMV reactivation (12).
The definitive diagnosis of CMV colitis is made by demonstrating CMV in tissue with the appearance of macroscopic mucosal lesions in a patient with upper and/or lower gastrointestinal symptoms. Viral culture, virus isolation, histopathology, IHC, or DNA hybridization can be used to investigate the presence of CMV in tissue. Demonstrating the presence of CMV DNA through nucleic acid tests or antigenemia tests in the blood is insufficient for the definitive diagnosis of CMV gastrointestinal disease (13). The plasma CMV PCR test is a non-invasive test that detects CMV viremia, which may be associated with CMV gastrointestinal disease. However, studies investigating the use of plasma CMV PCR for the diagnosis of CMV colitis are inconsistent. This study aimed to compare patients with CMV infection who presented with IBD exacerbation, evaluate them in terms of diagnosis and treatment, and investigate the importance of CMV DNA levels in terms of colitis development.
Materials and Methods
Patients who were followed up with a diagnosis of IBD and were examined with a preliminary diagnosis of CMV colitis at a university hospital between January 2016 and December 2021 were retrospectively scanned using the hospital’s electronic medical records. Demographic characteristics of the patients (age, gender, comorbidities) and information about IBD (year of diagnosis, treatment history related to the disease) were collected. The study included patients aged 18 years and older for whom demographic and clinical data were available. Patients who did not have data on antiviral treatment, were not tested for serum CMV DNA PCR, or did not undergo histopathological examination for CMV colitis were excluded. In this retrospective study, patients were categorized into two groups: Patients with CMV colitis diagnosed histopathologically and patients without CMV colitis.
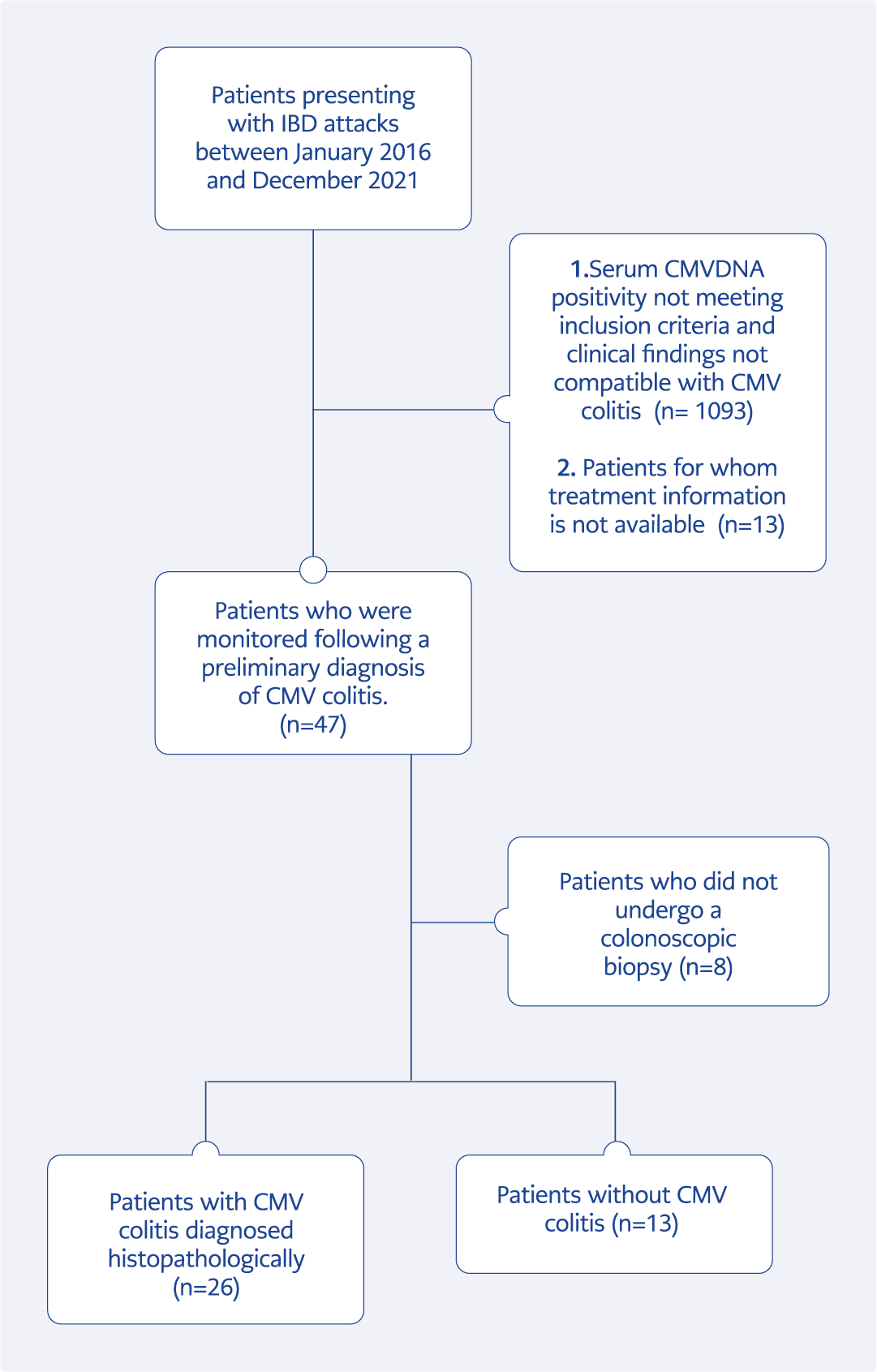
Figure 1. Flow chart of patients with inflammatory bowel disease who were examined for CMV infection within the study period.
Patients diagnosed with CMV colitis according to pathological criteria and confirmation by anti-CMV antibody positivity on immunohistochemical analysis as a result of the biopsy taken from lesions suspicious for CMV infection by colonoscopic sampling were classified as the CMV colitis group; patients whose histopathologically CMV negative were classified as patients without CMV colitis. CMV DNAemia was defined as a serum CMV DNA PCR level was above 1000 copies/mL or above 500 copies/mL, and progressively increasing (Figure 1). Demographic data, clinical findings, and treatment results were compared between the two groups.
Serum CMV DNA was measured using the artus CMV PCR Kit CE (Qiagen N.V., Germany) on the QIAsymphony Instrument (Qiagen N.V., Germany). Ankara University School of Medicine Ethics Committee approved the study on May 5, 2022 with decision number 2022000280-2.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 23.0 (IBM Corp., Armonk, NY, USA). The variables were investigated using visual and analytical methods Shapiro-Wilk to determine whether or not they are normally distributed. Descriptive analyses were presented using means and standard deviations for normally distributed variables, median (min-max) for non-normally distributed variables, and frequencies for ordinal variables. The differences between the groups were investigated using the Student’s t-test or Mann-Whitney test according to normal or non-normal distribution. The chi-square test or Fisher’s exact test was used to compare categorical variables in different groups.
Results
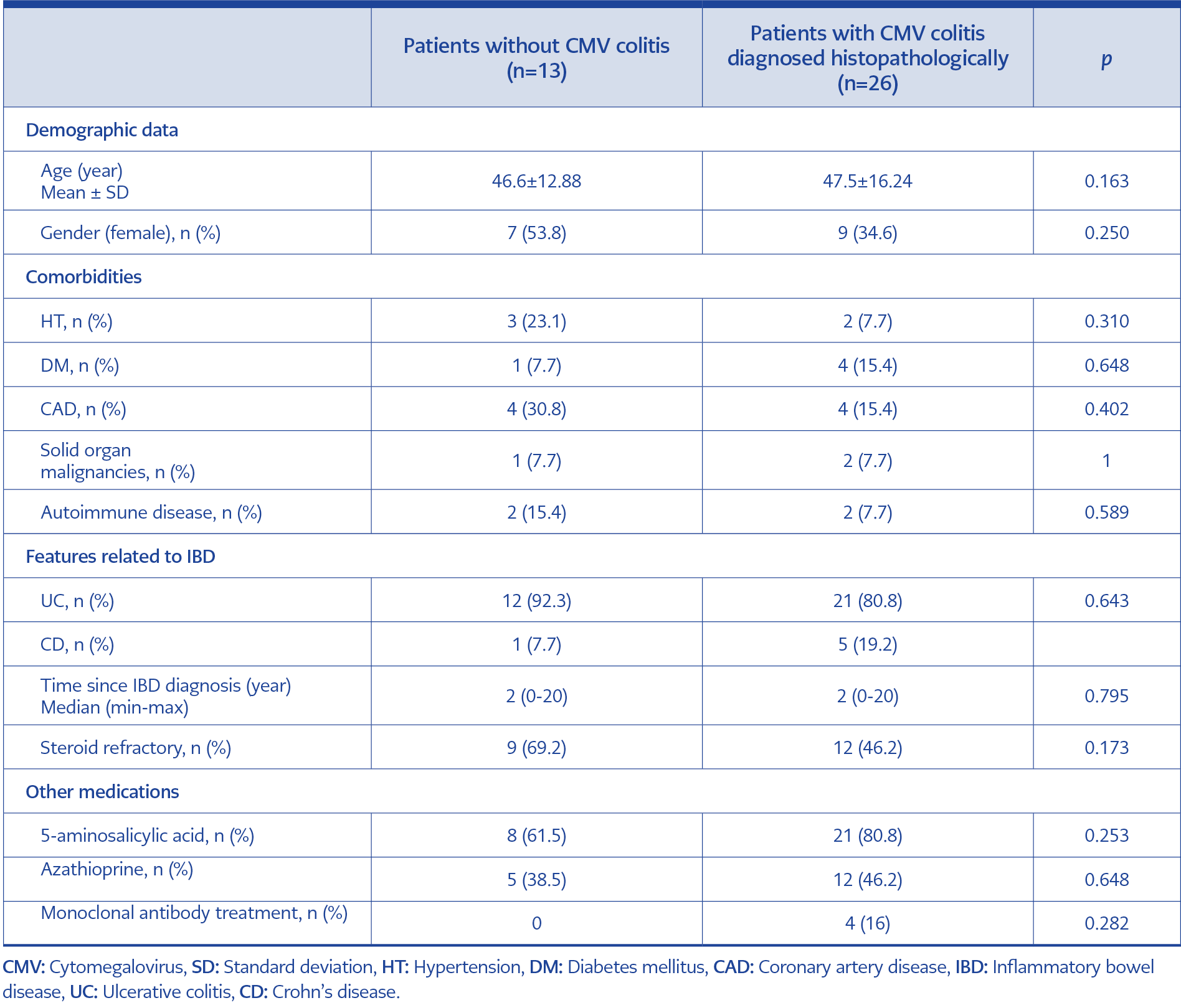
Table 1. Comparison of demographic and clinical characteristics of patients with a preliminary diagnosis of CMV colitis (N=39).
A total of 39 IBD patients, 33 (84.6%) with ulcerative colitis and 6 (15.4%) with Crohn’s disease, who were investigated preliminary diagnosis of CMV colitis and underwent colonoscopy, were included in the study. Of the patients, 16 (41%) were women, the median age was 47 (22-74). 11 (28%) patients had at least one accompanying disease. The most common comorbidities were hypertension, coronary artery disease, and diabetes mellitus. Other than IBD, 4 (%10.3) patients had additional autoimmune diseases, and 5 (12.8%) had malignities (Table 1).
The most common clinical symptoms were bloody diarrhea (64%), abdominal pain (38.5%), weight loss (38.5%) and fever (30.8%). There was an average of four years between IBD diagnosis and the diagnosis of CMV infection. In the year of IBD diagnosis, 12(30.8%) patients had CMV infection, and 21(53.8%) were unresponsive to steroid treatment. Apart from steroids, the most frequently used drugs for IBD by patients were 5-aminosalicylic acid 29(74.4%) and azathioprine 17(43.6%). 4(10.8%) patients were receiving monoclonal antibody therapy.
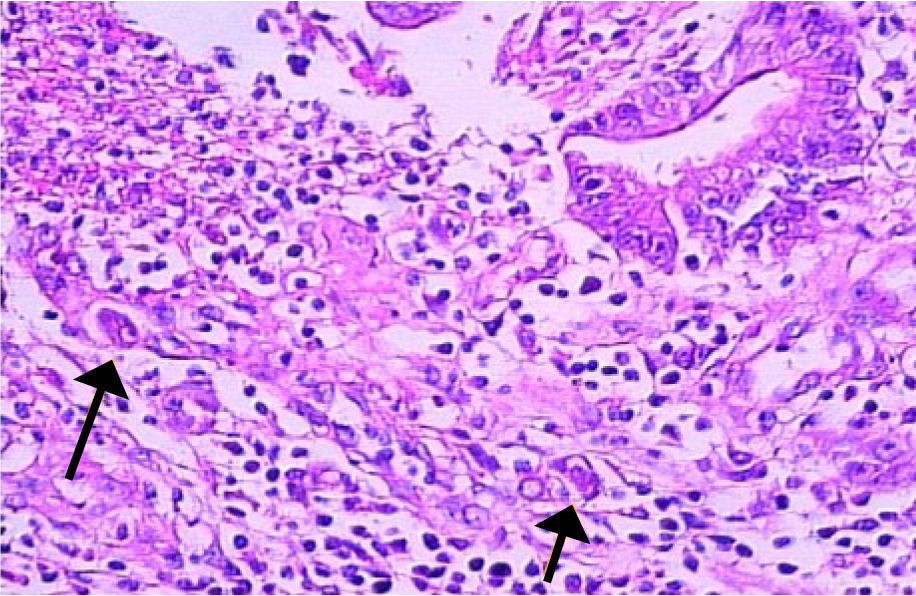
Figure 2. Endothelial cell nuclei with cytomegalic changes and intranuclear viral inclusions (H&E; x200).
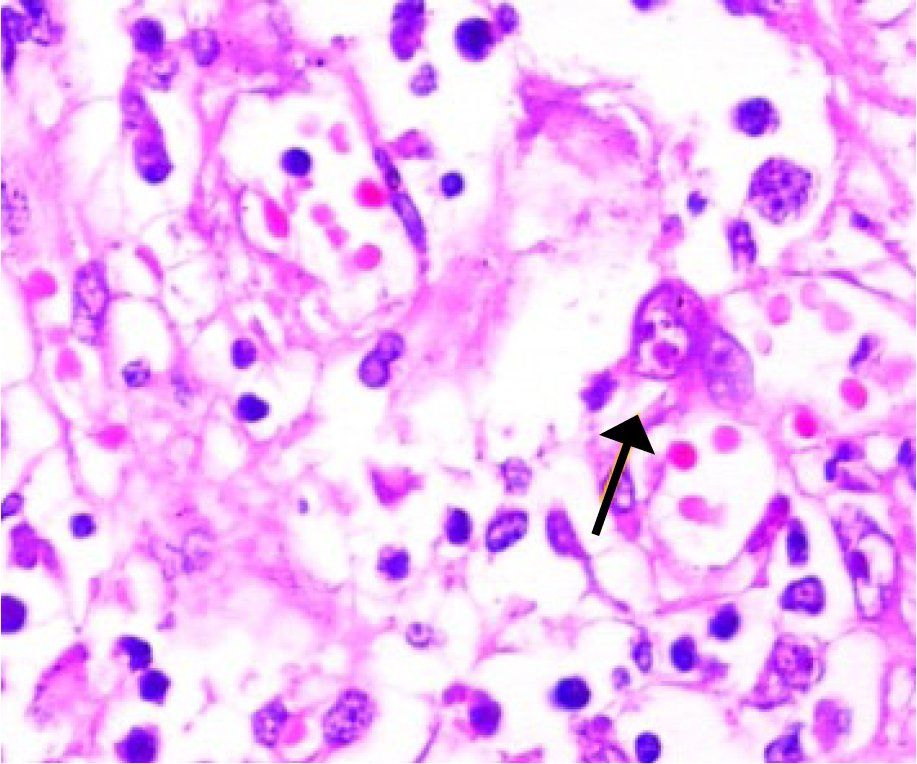
Figure 3. Owl’s eye intranuclear viral inclusion in an endothelial cell (H&E; x400).
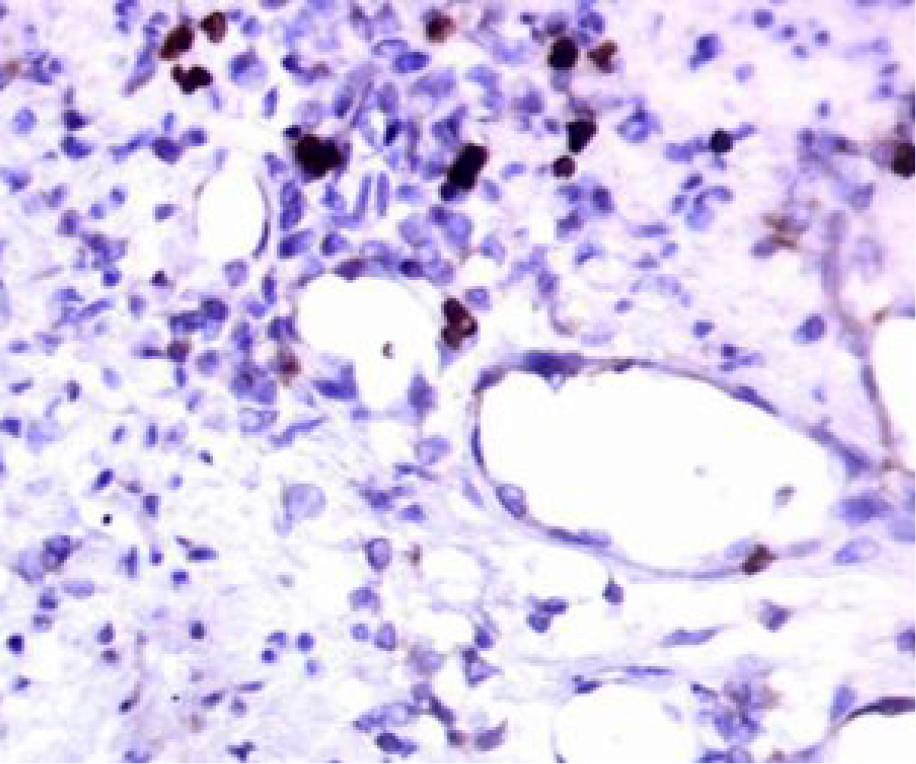
Figure 4. Positive cells with anti-CMV immunohistochemistry (IHC; x200).
A colonoscopy was performed on all patients with suspicion of CMV colitis. In 13 (33.3%) patients, CMV presence could not be demonstrated during colonoscopy, and these patients were classified as the patients without colitis. The most common pathological findings in 26 (66.7) patients diagnosed with CMV colitis were diffuse active colitis characterized by inflammatory granulation tissue development at the ulcer base, crypt distortion, crypt abscess, and cryptitis. The rectosigmoid region was most commonly involved. The presence of CMV was demonstrated by both H&E (Figures 2 and 3) and IHC (Figure 4) in CMV colitis patients. One patient in the CMV colitis group had CMV colitis six years ago and received antiviral treatment at that time.
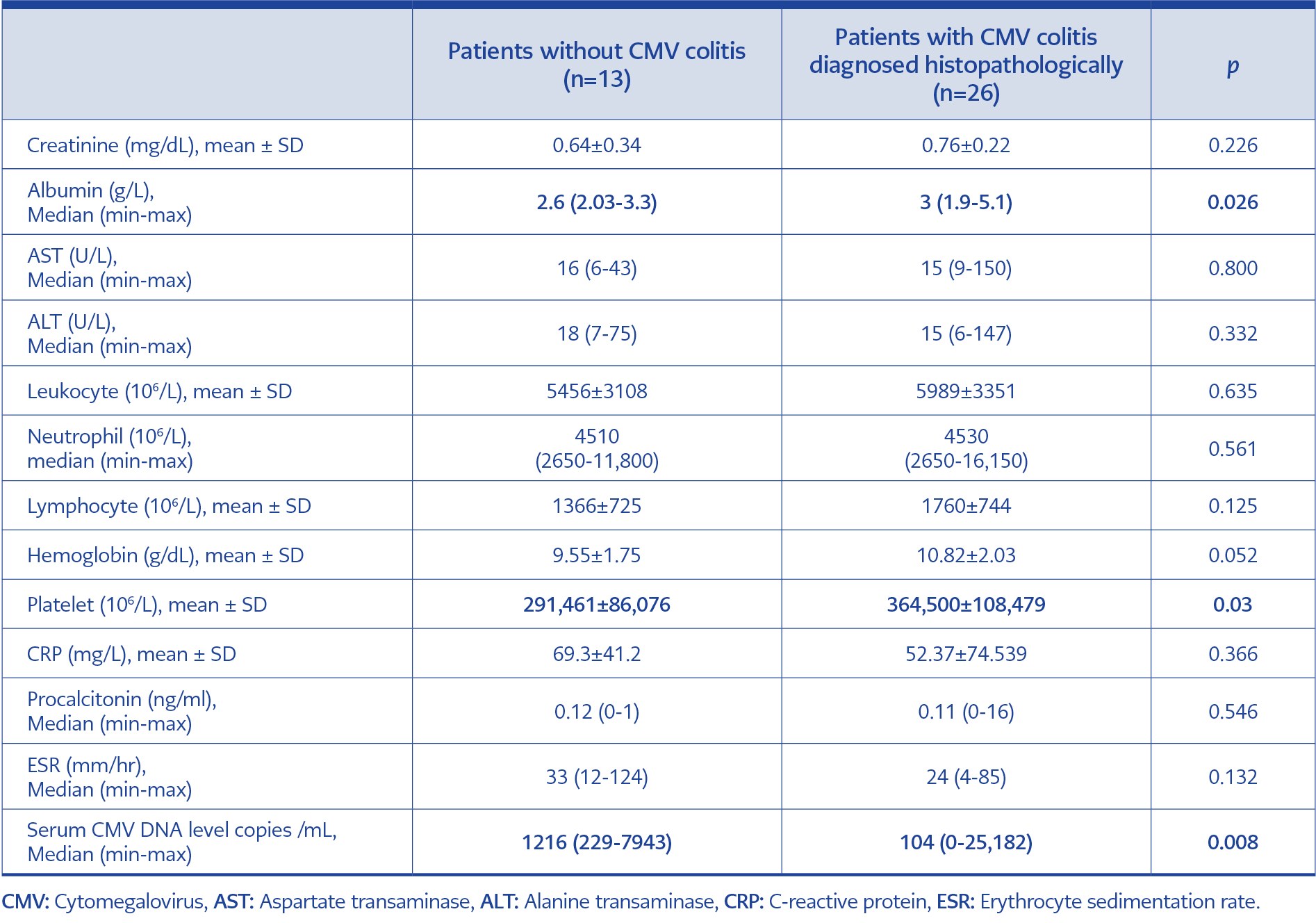
Table 2. Comparison of laboratory parameters of patients (N=39).
No significant difference was detected regarding demographic and IBD-related characteristics between the patients with CMV colitis diagnosed histopathologically and those without CMV colitis. In the comparison of laboratory parameters between the two groups, albumin and platelet levels were statistically significantly higher in the CMV colitis group (p=0.026, p=0.03 respectively) (Table 2).
In the group of patients with CMV colitis, ten patients had elevated serum CMV DNA PCR levels, which met the criteria for CMV DNAemia. However, 16 out of 26 patients did not have concomitant CMV DNAemia, and ten patients had a serum CMV DNA PCR level of zero. The median CMV DNA level in patients with isolated CMV DNAemia was 1216 copies/mL, which was significantly higher than the 104 copies/mL found in patients with CMV colitis (p=0.008).
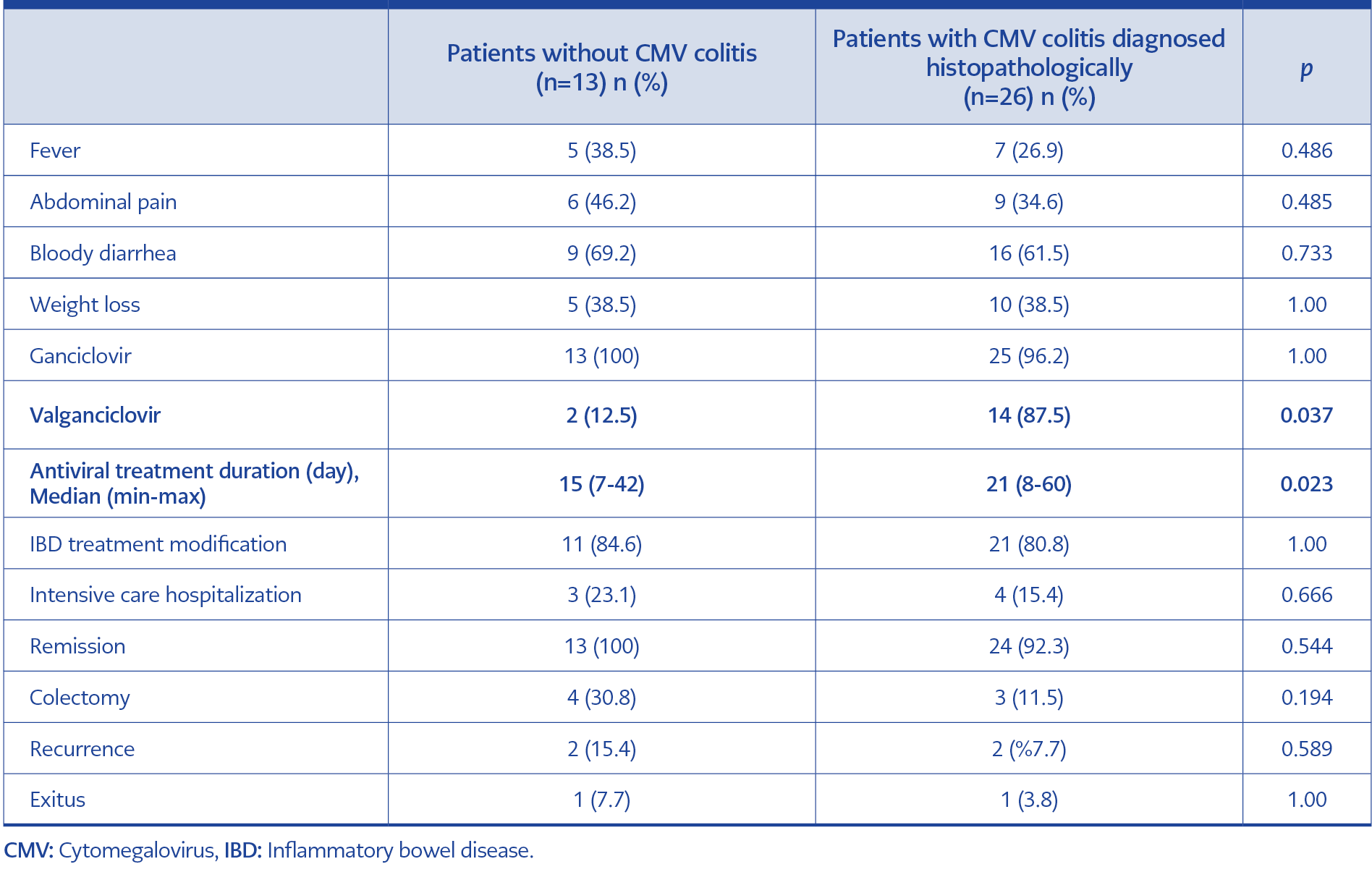
Table 3. Comparison of clinical presentation, treatment, and outcomes (N=39).
All patients included in the study were hospitalized and received antiviral treatment. Treatment began with ganciclovir for 38 patients, and 15 of them continued with maintenance treatment using valganciclovir. One patient in the CMV colitis group declined ganciclovir treatment, opting for valganciclovir instead, and showed improvement after 30 days of treatment. The duration of treatment was significantly longer in the CMV colitis group (median 21 vs. 15 days; p=0.023). The rate of switching to valganciclovir maintenance therapy was notably higher in the CMV colitis group (p=0.037) (Table 3).
A total of 32 (82.1%) patients underwent a modification of their immunomodulatory treatment regimen during or after CMV infection. Totally 7 (17.8%) patients underwent colectomy (two because of colonic perforation and one because of toxic megacolon). The need for intensive care developed in 7 (17.9%) patients; 2 (%5) patients died, one because of septic shock after colectomy and the other because of acute coronary syndrome.
Four patients had recurrent CMV infection after an average of 2.5±1.7 years. There was no statistically significant difference between the two groups regarding remission, progression to colectomy, recurrence and mortality.
Discussion
From the first case reported in 1961 of a CMV inclusion body in the colon pathology of a patient with ulcerative colitis to the present day, the clinical significance of CMV reactivation for IBD patients remains unclear (14). However, it is crucial to exclude CMV reactivation that may accompany treatment-resistant patients with IBD exacerbation (6, 15-18). Some studies indicate that CMV infection is a poor prognostic factor in patients with IBD (19, 20). It was demonstrated that antiviral treatment initiated for CMV infection reduces the necessity for colectomy due to unresponsiveness to medical treatment (21). On the other hand, some studies indicate that the disease can progress regardless of antiviral treatment (22, 23). Previous studies on this topic were mainly retrospective, involved small groups, and examined CMV infection using different definitions, making it challenging to assess the impact of CMV infection on IBD patients from a clinical perspective.
In patients with IBD, CMV disease was more frequently reported in the group treated with steroids compared to the steroid-naïve group. This was also more prevalent during the active disease period compared to the inactive period. It is unclear whether steroid use increases the risk of CMV colitis or is just a sign of severe disease. Nevertheless, in vitro studies have shown that steroids can suppress CMV-specific T-cell functions in a dose-dependent manner (24). Supporting previous similar studies, 53.8% of the patients in our study were unresponsive to steroids. However, no significant difference was found in the rates of steroid-resistant patients between the groups with between the groups with and without CMV colitis.
Because colonoscopic biopsy, the gold standard for diagnosing CMV colitis, takes time, developing alternative and/or complementary diagnostic algorithms with faster tests, such as CMV antigen or CMV DNA PCR, is crucial to prevent clinical deterioration in patients through early treatment. Serum PCR test results may be negative in approximately 25% of CMV-related gastrointestinal pathologies (25). When the cut-off value was set at 1150 copies, the sensitivity of blood CMV DNA PCR in predicting CMV colitis was 44.4%, and the specificity was 78.9% (26). In the study by Kim et al. including 229 patients, 83 of whom were diagnosed with CMV colitis in the presence of a significant ulcer, CMV antigen positivity (33/50 [66.0%] vs. 31/102 [30.4%]) and blood CMV PCR positivity (25/37 [67.6%] vs. 24/86 [27.9%]) were found to be significantly higher in the CMV colitis group. However, if the ulcer is not apparent, although CMV antigenemia and blood CMV PCR tests have high specificity in diagnosing CMV colitis, their sensitivity was found to be low (27). In the study by Ozdemir et al., CMV DNA PCR was found to be negative in the blood of 66.6% of the patients with CMV DNA PCR positivity in the colon mucosa (28). Even though there have been recommendations to use PCR with samples other than tissue for diagnosing CMV colitis, recent studies suggest that a negative plasma CMV PCR test alone may not be enough to rule out colitis. However, if both the plasma and stool CMV DNA PCR tests are negative, the diagnosis of CMV colitis can be ruled out (29). In our study, serum CMV DNA was detected at negative or low levels in 16 patients with CMV colitis (median level was 104 copies /mL). Therefore, a low serum CMV DNA level is an insufficient criterion for excluding CMV colitis.
Our study was handled with a multidisciplinary approach, including gastroenterology, medical pathology and infectious diseases, at a tertiary university hospital. Compared to similar studies, the number of patients pathologically diagnosed with CMV colitis is relatively high. This study also has some limitations. First, this retrospective study was conducted on a limited number of patients and did not include a control group. Second, long-term outcome data could not be presented because of the short follow-up period and the inability to access all follow-up records. Third, since CMV DNA could not be studied in tissue samples in our hospital and there was a lack of data regarding the plasma antigen results of some patients, comparisons could not be made on these issues.
In conclusion, it is important to note that patients with IBD diagnosed with CMV colitis may not always have CMV viremia. As per our research, CMV colitis may be present even in patients with CMV DNA levels of <500. Thus, relying solely on serum CMV DNA is insufficient to rule out CMV colitis. Patients with high suspicion of CMV colitis, even if CMV DNA is negative or low titer, should be evaluated for colonoscopy and investigated for the presence of CMV in the tissue with immunohistochemical staining. In patients with IBD flare-ups, clinicians need diagnostic algorithms that can help them consider the possibility of CMV colitis and guide them toward appropriate invasive diagnostic tests. Analyzing CMV DNA in stool or tissue may expedite this process. Risk models should be created to reduce unnecessary treatment and invasive procedures. Prospective studies in which long-term clinical results can be monitored are needed.