Introduction
Central nervous system (CNS) infections can develop due to bacteria, viruses, and fungi (1). The most common cause is bacteria. Although fungal meningitis is rare, there has been an increase in the number of cases in recent years (2, 3). In the vast majority of CNS candidiasis, the primary site of infection is the lungs or skin, followed by direct or hematogenous spread to the CNS (4, 5). The most common opportunistic fungi in humans are Candida spp. (3). High-dose and long-term use of antibiotics, long-term immunosuppression conditions such as hematological malignancies, and solid organ or bone marrow transplants predispose to candidiasis (3, 6). It is estimated that 6% of patients with disseminated candidiasis will develop neuroinfection due to the biofilm formation of Candida spp., which protects yeast cells from microglial activity (3). This article presents a case of Candida meningitis accompanied by oral candidiasis in a patient diagnosed with ankylosing spondylitis (AS) and psoriasis who was on adalimumab therapy.
CASE

Figure 1. Findings of oral candidiasis in the patient.
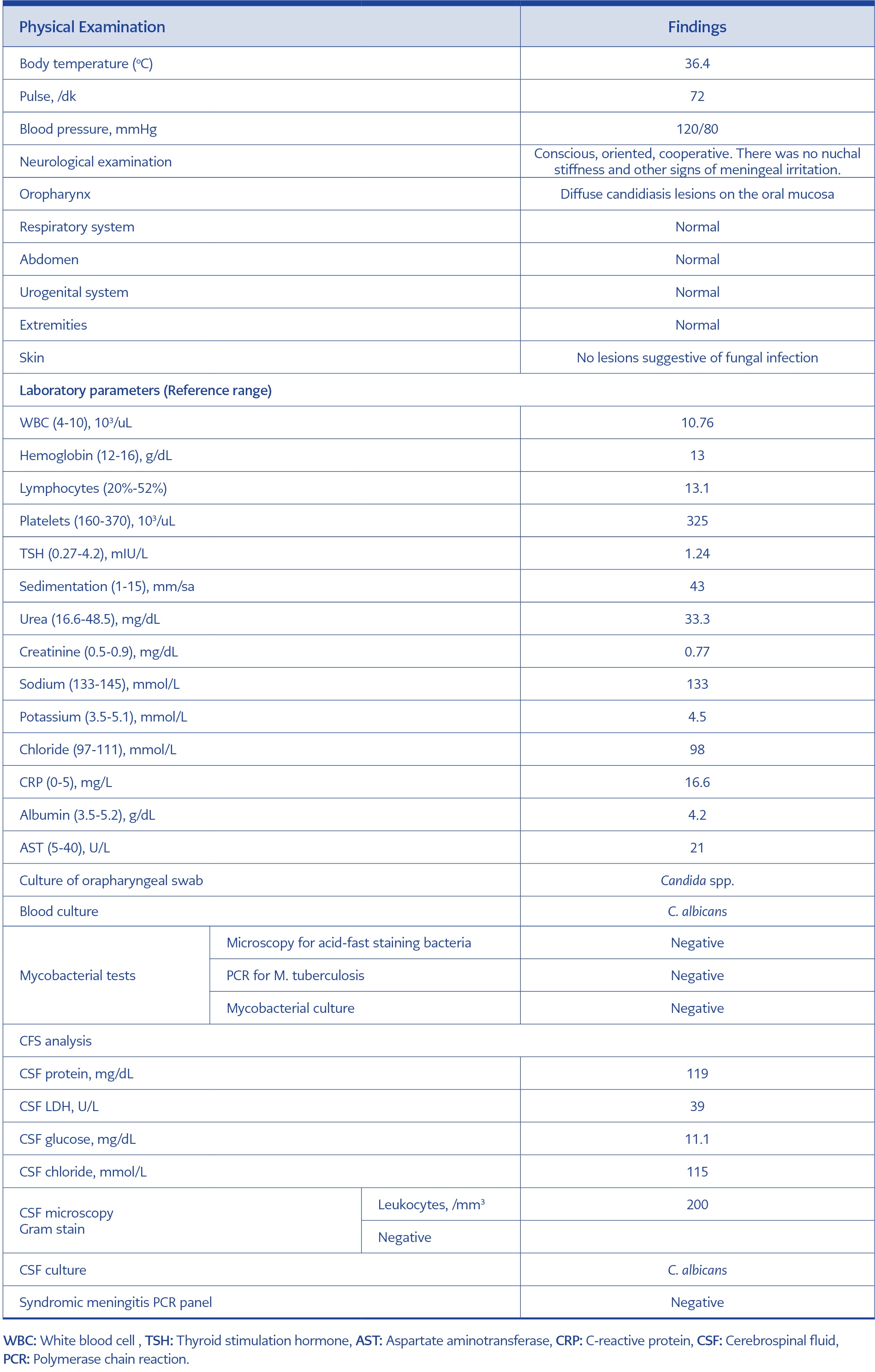
Table 1. Laboratory values and physical examination findings at the time of patient admission.
A 37-year-old female patient was admitted to the neurology department with a diagnosis of pseudotumor cerebri due to complaints of a constricting headache starting from behind both ears and spreading to the forehead, blurred vision, double vision, nausea, and vomiting that had developed over the past 15 days. Physical examination was normal except for lesions compatible with oropharyngeal candidiasis extending to the larynx level (Figure 1). She was fully conscious, oriented and cooperative with no signs of meningeal irritation. The patient underwent endoscopy, and white plaques suggesting Candida esophagitis were observed. An oropharyngeal swab sample was taken. The patient was on adalimumab therapy for psoriasis and AS. A lumbar puncture was performed. Cerebrospinal fluid (CSF) tests showed low glucose and high protein levels (Table 1). Thus, the patient was transferred to the Infectious Diseases Department with the diagnosis of meningitis and or encephalitis. Intravenous (IV) treatment with 2 g ceftriaxone q12h, 1 g vancomycin q12h and 750 mg acyclovir q8h was started. Oral care with bicarbonate was done. Oral nystatin therapy was also started. Her HIV serology was negative.
The patient remained afebrile, and the headache persisted on the third day of treatment. The patient’s brain magnetic resonance imaging (MRI) was normal. Because of bilateral papilledema observed in the fundoscopic examination performed for double vision, the patient was consulted by neurology, and diazomide treatment was initiated. Candida albicans grew in blood and CSF cultures; therefore, the patient’s treatment was changed to fluconazole 200 mg q12h and liposomal amphotericin B 250 mg q24h on the fifth day. On the second day of the antifungal treatment, the headache and nausea subsided, and by the fourth day, the double vision improved. By the end of the first week, oral lesions had completely healed, and there was no deterioration in the clinical condition. Control CSF analysis was recommended to the patient but could not be performed because the patient did not accept it. The treatment was continued for 28 days, and the patient was discharged in good health at the end of antifungal treatment. No recurrence was observed in the follow-up after discharge. Informed consent was obtained from the patient.
Discussion
Patients with rheumatic diseases are exposed to various risk factors that significantly increase the incidence of fungal infections. The use of broad-spectrum antibiotics can alter mucosal flora, leading to the proliferation of Candida spp., corticosteroids can affect the activity of polymorphonuclear cells, macrophages, and T cells, surgical procedures and the use of immunosuppressive drugs – especially biological agents – facilitate the spread of opportunistic pathogens (7, 8). Our patient was diagnosed with AS, and she was on adalimumab. Adalimumab is a recombinant monoclonal antibody and a tumor necrosis factor-alpha (TNF-α) inhibitor used in the treatment of various autoimmune conditions such as rheumatoid arthritis, AS, psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. TNF-α is a proinflammatory cytokine that plays a crucial role in the pathogenesis of many inflammatory diseases by stimulating the release of inflammatory cytokines such as interleukin 1 beta (IL-1β), IL-6, and IL-8 (9, 10). Approximately 80% of invasive fungal infection cases related to anti-TNF use are associated with infliximab, 16% with etanercept, and only 4% with adalimumab. These fungal infections primarily affect the lungs and include histoplasmosis (30%), candidiasis (23%), and aspergillosis (23%) (9).
Various Candida spp., including C. albicans, Candida tropicalis and Candida parapsilosis, can cause infections. The positivity rate of fungal cultures in CSF for Candida infection is approximately 80% (11). Typically, CSF analysis shows pleocytosis, low glucose, and high protein levels. The initial symptoms of Candida meningitis resemble those of bacterial meningitis, such as fever, headache, neck stiffness, and altered consciousness (11, 12). However, unlike bacterial meningitis, which typically presents acutely, Candida meningitis can have a more insidious onset and may progress in weeks, making diagnosis challenging. This clinical course can mimic tuberculous meningitis (13). Our patient did not exhibit confusion or neck stiffness on physical examination but had long-standing, severe headaches, blurred vision, and double vision.
Managing CNS infections caused by Candida is challenging, with a mortality rate of 10% to 30%, even with adequate treatment (11, 14). Liposomal amphotericin B, either alone or combined with flucytosine, is recommended for treatment. If a foreign body, such as a surgically implanted device, is present in the CNS, it should be removed due to biofilm formation. Amphotericin B has broad-spectrum antifungal activity and achieves high concentrations in the CNS. Fluconazole, which penetrates the CSF well and is well-tolerated with infrequent side effects, is another antifungal agent used in treatment (14). Although fluconazole or amphotericin B is mentioned in the treatment of Candida meningitis, dual antifungal use is also available in the current literature, and the current literature is mentioned in references and case reports. Since meningitis may be aggressive in our patient due to the growth of C. albicans in both CSF and blood cultures, fluconazole and amphotericin B were administered in combination (15, 16).
Conclusion
Patients receiving anti-TNF-α therapy must be closely monitored for serious and opportunistic infections. The clinical presentation of Candida meningitis may mimic tuberculous meningitis; therefore, it should be included in the initial differential diagnosis in these patients.