Introduction
The demographic shift with an aging population worldwide has highlighted the unique healthcare challenges the elderly face. According to the Turkish Statistical Institute data, the population aged 65 and over reached 8,722,806 in 2023, accounting for 10.2% of the total population (1). Population projections indicate that the proportion of the elderly population is expected to reach 12.9% in 2030, 22.6% in 2060, and 25.6% in 2080. Therefore, understanding the health needs of this demographic group is vital for the future planning of public health and healthcare services (2).
Bacterial infections present complex challenges in older adults, particularly those aged 80 years and above, due to multiple factors, including diminished immune function, chronic diseases, nutritional deficiencies, and increased risk of adverse outcomes. Reduced immunity often leads to unusual symptoms. This may result in the absence of specific symptoms or signs of infection, making the diagnosis more challenging for healthcare providers. Despite these challenges, timely and accurate identification of bacterial infections and effective antimicrobial treatment greatly improve patient outcomes (3-5).
Infections in individuals aged 65 and over become more frequent, depending on factors such as the weakening of the immune system with age, the prevalence of chronic diseases, and greater exposure to social care environments. In addition to the frequency of infections, response to treatment, and mortality rates in individuals over 65 differ from those in the younger age groups (6, 7). Multiple health problems increase the risk of infection, making treatment options and outcomes more complex. The growing elderly population necessitates the development of strategies to manage and treat infections.
Common infections in this age group include respiratory tract infections, urinary tract infections, skin infections, and viral diseases. Managing these infections is critical for maintaining general health and improving the quality of life of the elderly. Knowing the frequency of infections in this population can aid in managing these diseases (8). Early diagnosis and treatment of infections can reduce morbidity and mortality rates. Therefore, the frequency and characteristics of infections in this group are significant for developing effective prevention and treatment strategies. Studies focusing on the frequency and characteristics of infections in the elderly can contribute to developing more effective health policies and treatment protocols.
This study aimed to enhance the understanding of infectious diseases within the elderly population, a demographic with a growing number and vulnerability, by identifying and characterizing common acute bacterial infections. Understanding the spectrum of infection is crucial for effectively tailoring preventive and therapeutic measures.
Materials and Methods
Patients older than 65 years diagnosed with bacterial infection and received inpatient treatment between January 1, 2018, and December 31, 2022, in the Department of Infectious Diseases and Clinical Microbiology inpatient ward of our hospital -a 700-bed tertiary-level state hospital in Türkiye- were included in this single-center retrospective cohort study. Patients with non-infectious causes of their illness, younger than 65 years old, and lacking accessible medical records were excluded. Patients were divided into groups aged 65-79 (Group 1) and 80 and above (Group 2). The demographic, clinical, and laboratory characteristics, treatments, and mortality rates of the groups were compared.
Bacterial infections were defined according to the recommendations of the Centers for Disease Control and Prevention (CDC) (9). Patients were identified as having sepsis if they exhibited clinical criteria consistent with the sepsis-3 definition (10). Patients were considered septic if they demonstrated an increase in the Sequential Organ Failure Assessment (SOFA) score by 2 points or more, indicating organ dysfunction. Common clinical manifestations included changes in vital signs such as fever or hypothermia, tachycardia, tachypnea, hypotension, altered mental status, decreased urine output, and elevated serum lactate levels. Therefore, fever was classified as a central body temperature above 37.8 ºC upon admission. Skin and soft tissue infections are defined as foot infections and cellulitis.
The participants’ demographic details, clinical characteristics, laboratory findings, and radiological data were carefully documented using a uniform data collection sheet utilizing electronic health records. Laboratory values were assessed at admission, within 48/72 h of antibiotic administration, and on the last follow-up day. They were monitored thoroughly from admission to discharge or death. Their medical records were examined to evaluate various clinical attributes such as sex, age, and whether they were immunocompromised, along with presenting signs and symptoms such as fever, cough, production of sputum, difficulty urinating (dysuria), diarrhea, vomiting, nausea, alterations in consciousness and mental condition, the use of antibiotics, the requirement for intensive care, and the rates of mortality encountered within the hospital.
Comorbidities including diabetes mellitus (DM), hypertension (HT), chronic obstructive pulmonary disease (COPD), chronic heart disease (CHD), malignancy, the number of hospitalizations within a year, all medications taken during their hospital stay, duration of antibiotic therapy, intensive care unit (ICU) admission, and length of ICU stay were recorded. Polypharmacy is defined as the use of multiple medications by a patient, typically involving the use of at least five medications (11, 12).
Each patient underwent a physician assessment, and the primary healthcare provider determined the treatment plan. Additionally, routine blood examinations, including complete blood counts, serum biochemical tests, C-reactive protein (CRP) levels, procalcitonin measurements, and culture tests, were performed. Only one hospital admission for each patient was included in the study. Microorganisms were identified using a VITEK 2 automated system (bioMérieux, Marcy l’Etoile, France).
The primary endpoints included time to clinical improvement, discharge, or death. The primary outcome assessed was the infection rate on hospital admission. The results were presented according to the STROBE guidelines (13).
The study adhered to the principles of the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of Ankara Etlik City Hospital on June 12, 2024, with the number AEŞH-BADEK-2024- 373.
Statistical Analysis
The results were expressed as numbers (n) and percentages (%) for categorical variables, while continuous variables were presented as mean ± standard deviation or median (minimum-maximum). The normality assumption for continuous variables was assessed using the Kolmogorov-
Smirnov test. Categorical variables were analyzed using the chi-squared or Fisher’s exact test. Independent continuous variables between Group 1 and Group 2 were compared using either Student’s t-test or Mann-Whitney U test, depending on whether the statistical assumptions were met. The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 25.0 (IBM Corp., Armonk, NY, USA). Graphs were created using Microsoft Excel (2016). The statistical significance was set as p<0.05.
Results
Between January 1, 2018, and December 31, 2022, 185 patients diagnosed with bacterial infections were evaluated for eligibility in the study. Three patients without clearly defined infections and five patients with missing data during follow-up were excluded. Group 1, aged 65-79, comprised 63.3%, and Group 2, 80 years old and above, comprised 36.7% of the study population. Of the 177 patients included in the study, 98 (55.4%) were male and 79 (44.6%) were female. The mean age was 76.0 ± 8.8 years (range: 65-107).
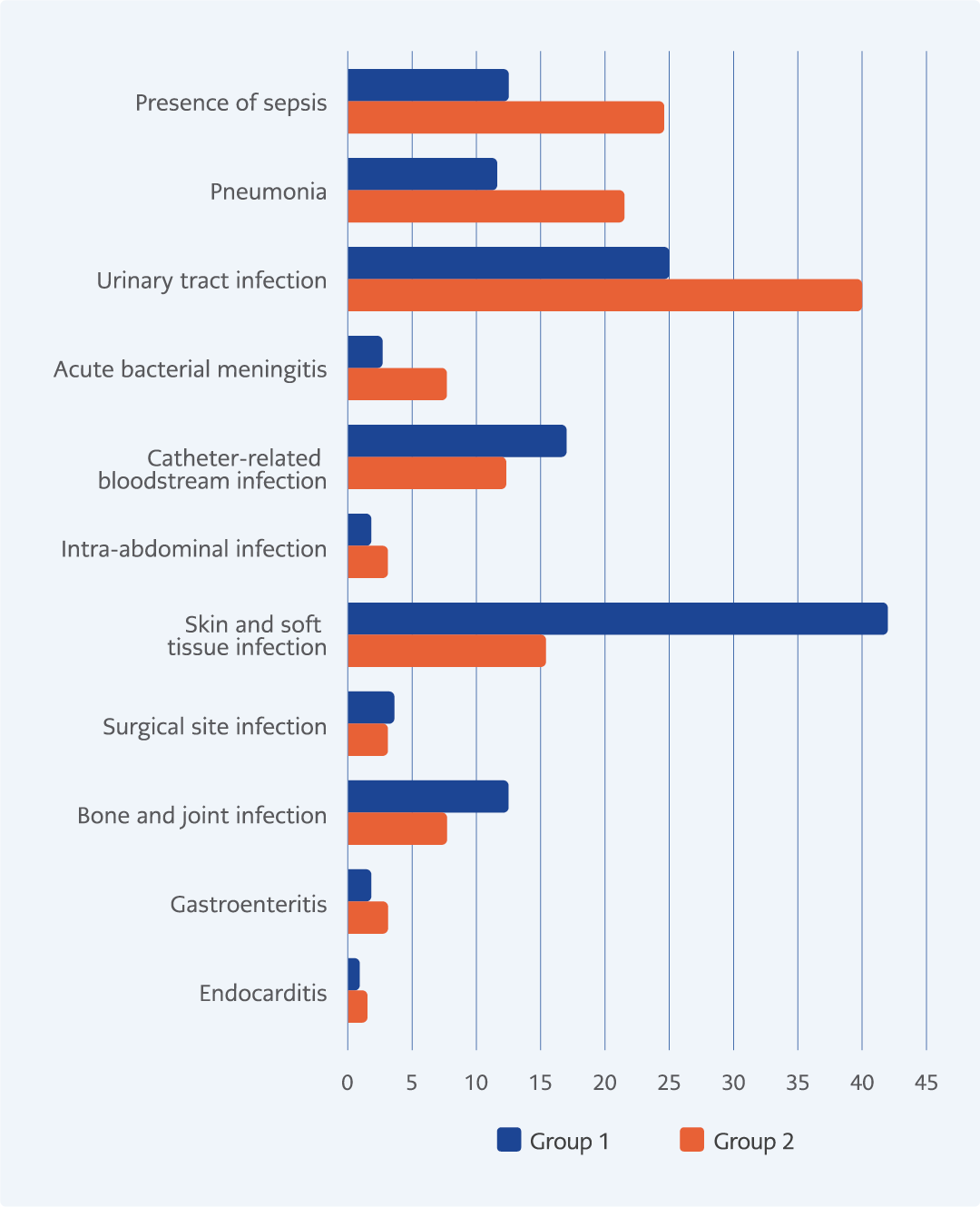
Figure 1. Distribution of infection types among elderly patients.
According to the guidelines (9), the types of infections observed in patients are detailed in Figure 1. The most common types of infections observed were skin and soft tissue infections (32.2%) and urinary system infections (30.5%), with 16.9% of patients also presenting with sepsis. Skin and soft tissue infections were the predominant reasons for hospital admission in Group 1, constituting 42% of cases. In contrast, Group 2 exhibited a significantly higher rate of urinary system infections and sepsis (p<0.001, p=0.037, and p=0.038, respectively). Prior to 2020, a total of 107 cases (60%) were monitored, comprising 14 cases (13.1%) of pneumonia, 35 cases (32.7%) of urinary tract infections, and 37 cases (34.6%) of skin and soft tissue infections. From 2020 to 2022, 70 cases (40%) were followed, including 13 cases (18.6%) of pneumonia, 19 cases (27.1%) of urinary tract infections, and 20 cases (28.6%) of skin and soft tissue infections. When comparing the rates of pneumonia, urinary tract infections and skin and soft tissue infections before and after 2020, the difference was not statistically significant (p=0.436, p=0.536, and p=0.403, respectively).
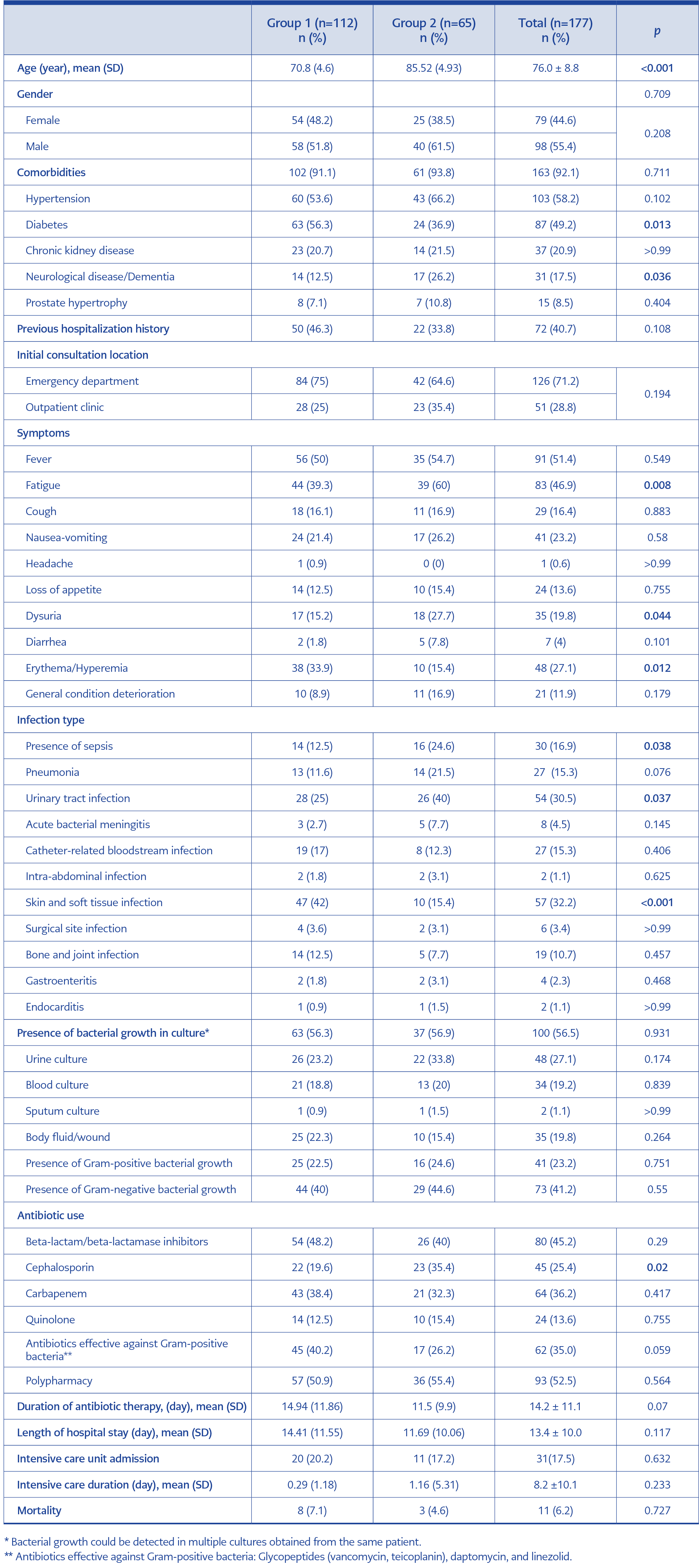
Table 1. Demographic and clinical characteristics, types of infections, and treatments of elderly patients.
The demographic and clinical characteristics, types of infections, and treatments of the patients are presented in Table 1. The most common symptoms leading to hospital admission were fever (51.4%), followed by fatigue (46.9%), and erythema (58.2%). Symptoms, such as fatigue and dysuria, were more frequently encountered in Group 2 (p=0.008 and p=0.044, respectively), whereas erythema was significantly more common among patients in Group 1 (p=0.012). Comorbidities were present in 161 (92.1%) patients, with HT being the most common (43.7%), followed by DM (49.2%). As shown in Table 1, DM (56.3%) was more prevalent in Group 1 (p=0.013), whereas neurological diseases/dementia were more common in Group 2 (p=0.036).
Of the patients, 126 (71.2%) initially presented to the emergency department, and 72 patients (40.7%) had a readmission history within one year. The mean duration of hospital stay was 13.4 ± 10.0 days, ranging from 2 to 55 days. Ninety-three (52.5%) patients received multidrug treatment (polypharmacy). During follow-up, 31 (17.5%) patients were transferred to the ICU. The mean ICU stay was
8.2 ± 10.1 days (range: 1-30). No notable differences were observed between the duration of the hospital stay and the treatment period.
Antibiotic treatments administered to the patients are detailed in Table 1. On average, all patients received antibiotics for 14.2 ± 11.1 days. During follow-up, 80 (45.2%) patients received beta-lactam/beta-lactamase inhibitors, 64 (36.2%) received carbapenems, 45 (25.4%) received cephalosporins, 24 (13.6%) received quinolone group antibiotics, and 62 (35.0%) were treated with antibiotics effective against Gram-positive bacteria. Some patients received antibiotics from more than one group. Beta-lactam/beta-lactamase inhibitors were the most commonly used in all groups; however, cephalosporin antibiotics were more frequently preferred in Group 2 patients (p=0.02).
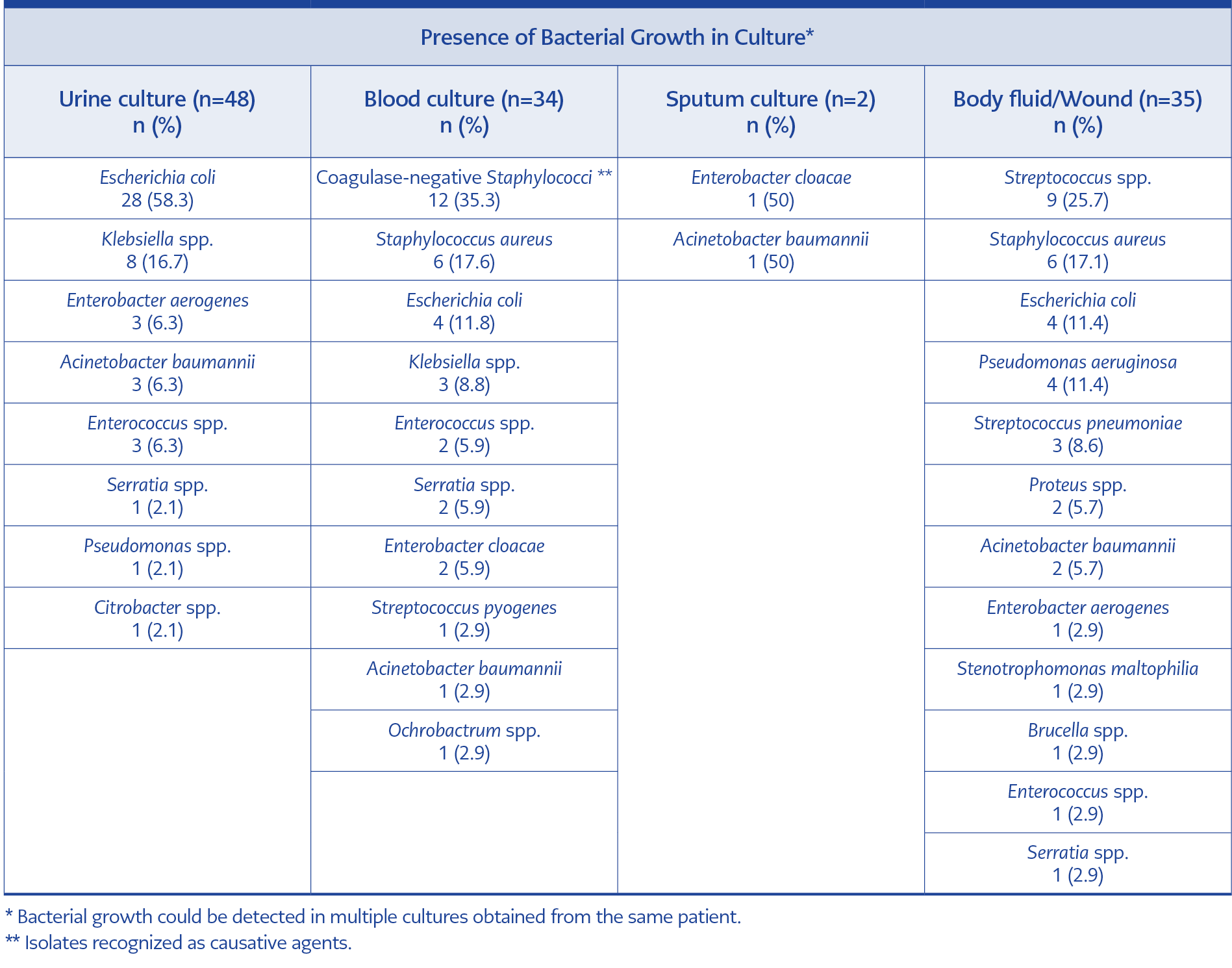
Table 2. Distribution of bacterial growth in culture samples.
A positive specimen culture was found in 100 (56.5%) patients. The most frequent positive culture growth occurred in 48 (27.1%) urine samples, followed by body fluids in 35 (19.8%) and blood samples in 34 (19.2%) (Table 2). Cases of growth in different types of cultures from the same patient (such as blood or sputum, blood, or urine) were present. There was no statistically significant difference in the positive culture growth between the groups.
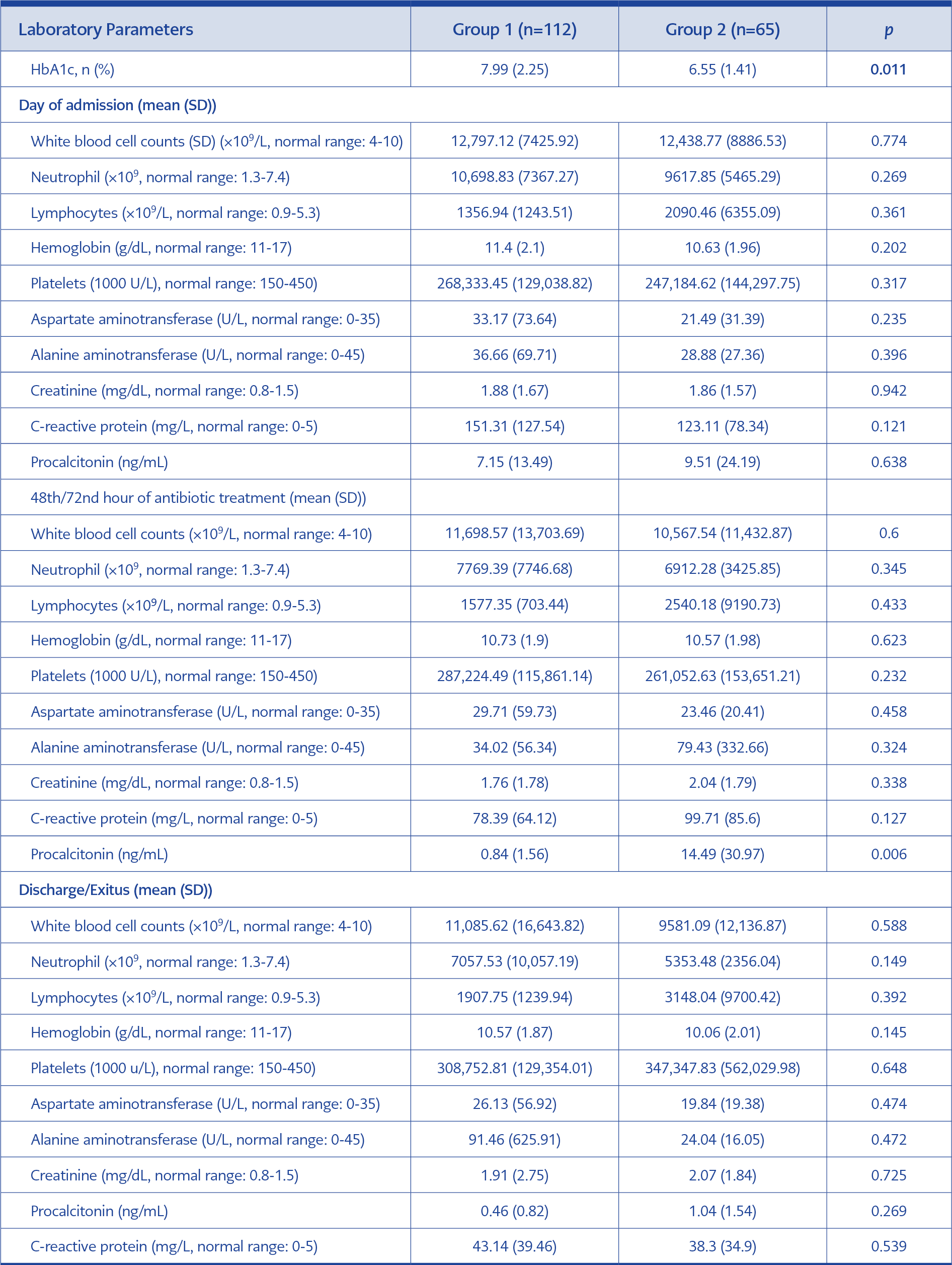
Table 3. The comparison of the laboratory findings in elderly patients.
Table 3 summarizes the laboratory parameters at admission, within 48/72 hours of antibiotic administration, and on the last follow-up day (discharge or death) between Group 1 and Group 2. A comparison of admission day parameters between the two groups revealed that HbA1c levels were higher in Group 1 (p=0.011). Additionally, a delayed procalcitonin response to antibiotic treatment was observed in Group 2, although no significant differences were detected in other laboratory parameters (p=0.006).
Discussion
The average age of the population is increasing, and the fastest-growing segment comprises individuals over the age of 80 years. This study evaluated the demographic and clinical characteristics, infection types, treatment preferences, and laboratory outcomes of elderly patients diagnosed with bacterial infections over a five-year period. Demographic analysis showed a high prevalence of comorbidities among the study population, with HT and DM being the most common. Notably, DM was significantly more prevalent in the younger elderly group (Group 1), while neurological diseases, such as dementia, were more common in the older group (Group 2). This distinction may influence the management strategies and outcomes of these patients. Studies conducted in our country with geriatric patient populations have similarly found that the prevalence of underlying diseases has increased in the geriatric population, with HT and DM being the most commonly detected comorbidities (5, 14, 15). The frequency of infection can also vary depending on the underlying diseases observed (16, 17). The rate of readmission and initial presentation in the emergency department highlighted the ongoing challenges in managing elderly patients with bacterial infections. These factors emphasize the importance of robust discharge planning and follow-up care to prevent readmissions, particularly for those with multiple comorbidities and advanced age.
The overall mortality rate in our study was 6.2% (11 cases), which may appear low despite the study population consisting of elderly patients. According to national data from Türkiye, mortality rates in elderly populations, particularly those with significant comorbidities, can vary widely. Our study’s rate is consistent with some hospital-based studies in the country that report mortality rates ranging between 5% to 20%, depending on the severity of the cases and the underlying conditions (1,18,19). Compared to the general elderly population’s mortality rates during similar study periods, our findings align more closely with elderly patients.
In our study, infection types varied between the groups. The most common causes of hospital admission were skin and soft tissue infections in Group 1, while urinary system infections and sepsis rates were higher in Group 2. Functional disabilities and neurogenic disorders, along with bladder outlet obstructions caused by prostate hypertrophy in males, can contribute to urinary retention. This retention may facilitate the colonization and proliferation of microorganisms. Furthermore, the laboratory results underscored the metabolic challenges in managing diabetes in the elderly, as demonstrated by higher HbA1c levels, indicating poorer glycemic control in Group 1, potentially contributing to their higher susceptibility to skin and soft tissue infections.
Studies in the literature show that urinary tract infections and skin and soft tissue infections frequently result in hospital admissions, similar to our findings. Lower respiratory tract infections are also commonly encountered. Notably, research conducted in intensive care settings has reported an increased incidence of pneumonia and bloodstream infections (5, 15, 20, 21). These findings highlight the need for targeted surveillance and preventive strategies tailored to the specific vulnerabilities of different age groups within the elderly population.
In our study, fever was the most common symptom at presentation, observed in approximately half of the patients, followed by fatigue, nausea, and vomiting. Notably, patients aged 80 years presented to the hospital with fatigue and urinary symptoms. Up to 50 per cent of older adults may not exhibit fever, even when facing severe infections (22). Similar to our findings, previous studies have also reported a lower incidence of fever (23, 24). It should be noted that fever may not always be present in elderly patients, which is present at outpatient clinics or emergency departments, even when an infection exists.
We found that the most common emergency department visits were by elderly patients, and approximately one-fifth of them had sepsis at admission. This situation was more prevalent in the older patient group (Group 2), underscoring the critical nature of timely and appropriate antibiotic treatment in these patients. The lack of prominent symptoms may be associated with disease severity progression in this demographic. A previous study also reported that nearly half of the patients over 65 years who were followed for an infection diagnosis were found to have sepsis (16). The average duration of hospital stays was 13.4 days (range: 1-55 days), and 17.5% of patients were transferred to the ICU in managing severe infections. In studies evaluating geriatric patients from the community, the average hospital follow-up duration was similar (15, 24).
Our study’s antibiotic treatment data revealed a nuanced approach to antibiotic administration, where beta-lactam/beta-lactamase inhibitors were most commonly used in all cases. In a multicenter study by Kurtaran and colleagues (5), in which the mean age was 75.1 ± 7.2 years, cephalosporins were the most frequently chosen antibiotic therapy, followed by beta-lactam/beta-lactamase inhibitors. Similarly, in our study, cephalosporins were the most commonly preferred antibiotics among patients in Group 2. This preference is thought to depend on the type of infection and the individual assessment of patients.
The culture positivity rate was 56.5%, and the most common source of microbial growth was urine samples, followed by body fluids and blood. The distribution of positive cultures suggests a high incidence of urinary tract infections, which are notably common and problematic in elderly populations due to factors such as neurological bladder and underlying urological conditions. Importantly, we found no significant differences in positive culture growth between the groups, suggesting that the microbiological profile of infections might be similar across different elderly subpopulations despite differences in clinical presentations and outcomes. This could imply that while the type and severity of infections differ, the causative agents remain consistent, allowing for a broad-spectrum initial antibiotic approach until the culture results guide specific therapies.
Various studies from our country have indicated that the most frequent bacterial culture positivity, similar to our study, occurs in urinary system infections (15, 23). In diagnosing infections among elderly patients, clinicians face challenges due to age-related physiological alterations, lack of conventional symptoms, such as fever, and the presence of comorbidities that complicate physical evaluations (25). Consequently, laboratory values may be crucial in guiding diagnostic decisions in this patient cohort. Studies have indicated that procalcitonin levels are more effective than CRP levels and white blood cell (WBC) counts in diagnosing bacterial infections (26-28).
In our study, the laboratory parameters showed that HbA1c levels were significantly higher in Group 1, suggesting poorer glycemic control, a known risk factor for infection severity and poor outcomes. The delayed procalcitonin response observed in Group 2 may be related to age-associated impairment in renal function. However, by the end of treatment, procalcitonin levels were similar between the two groups.
Our study has some limitations. First, focusing on a specific age group within a single geographical location may have limited the applicability of our results to a broader demographic group. Second, lacking a healthy control group may have restricted our ability to conduct robust comparative analyses. Also, details, such as the presence of urinary catheters and susceptibility profiles of the cultured bacteria, were not recorded. Additionally, using retrospective medical records as data may have led to biases or missing details about the patient’s medical histories, treatments, and recovery progress. The absence of long-term follow-up data may have restricted our understanding of the sustained effectiveness of treatment outcomes over time.
In conclusion, the findings illustrate the complex interplay between age, comorbidities, and clinical presentation in managing infections in the elderly. Our study highlights the challenges in diagnosing infections in the geriatric population, in which typical symptoms are often not observed, but non-specific symptoms are common. Notably, the increased rates of urinary system infections and sepsis in individuals over 80 years of age underscore the need for vigilant clinical oversight. Furthermore, effectively managing underlying conditions, such as diabetes, could significantly reduce the incidence of infections in this vulnerable group, emphasizing the critical role of comprehensive care strategies in improving health outcomes for elderly patients.