Introduction
Human bocavirus 1 (HBoV1) was first identified in 2005 through the molecular screening of respiratory tract samples and linked to lower respiratory tract infections in children in Sweden (1). It is a member of the Parvoviridae family and has been associated with a range of clinical presentations, from mild common colds to severe lower respiratory tract infections (2). Despite its high prevalence among children, there is limited data on HBoV1 infection in adult patients who were immunocompromised individuals (3-5). In a prospective cohort of 299 adult patients with a diagnosis of lower respiratory tract infection, having an 81% immunocompromised rate, the prevalence of HBoV1 using polymerase chain reaction (PCR) in bronchoalveolar lavage (BAL) materials was reported as 3.1% (6). In this report, we present a case of an immunocompetent adult patient with community-acquired HBoV1 infection complicated by myositis, resulting in respiratory failure.
Case
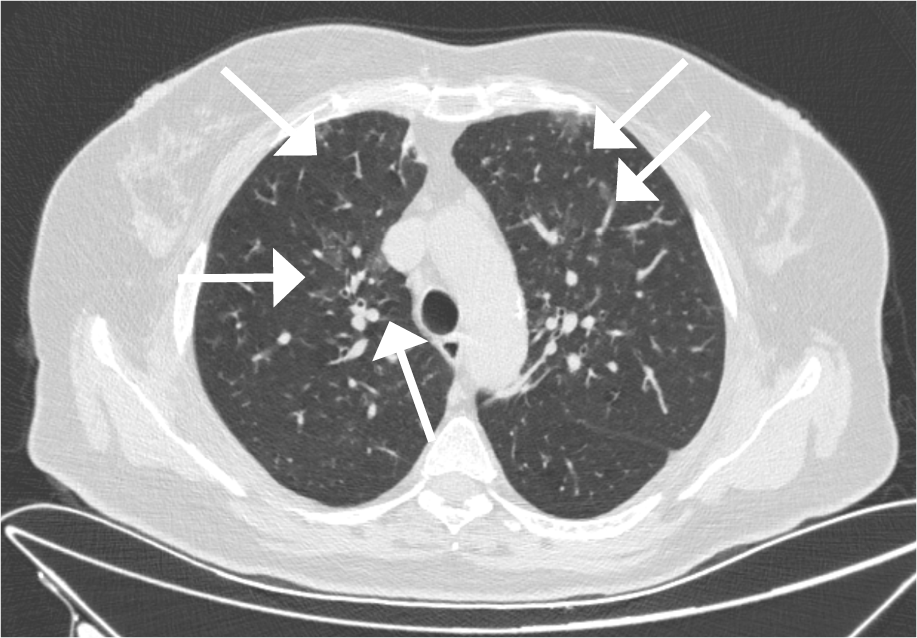
Figure 1. Thoracic computed tomography (CT).
A 61-year-old female patient with a history of coronary artery disease and essential hypertension was presented to our clinic with complaints of non-productive cough, low-grade fever, and nasal discharge lasting four days. On her initial physical examination, the patient exhibited decreased respiratory effort with the use of accessory respiratory muscles, abdominal breathing, tachypnea, and prolonged expiratory wheezes. The arterial blood gas analysis revealed hypercapnic respiratory failure with a pH of 7.30 and a carbon dioxide (pCO2) pressure of 68 mmHg. Therefore, she was intubated and followed on mechanical ventilation. She was admitted to the intensive care unit with an acute physiology and chronic health evaluation II (APACHE II) score of 17, indicating an expected mortality rate of 26%. Thoracic computed tomography (CT) revealed bilateral, multifocal, patchy ground glass opacities primarily affecting the upper zones, with no central or peripheral selection observed in the axial plane (Figure 1). These findings were accompanied by bronchi and bronchioles wall thickening, centrilobular nodules forming a tree-in-bud pattern, and mosaic perfusion due to air trapping.
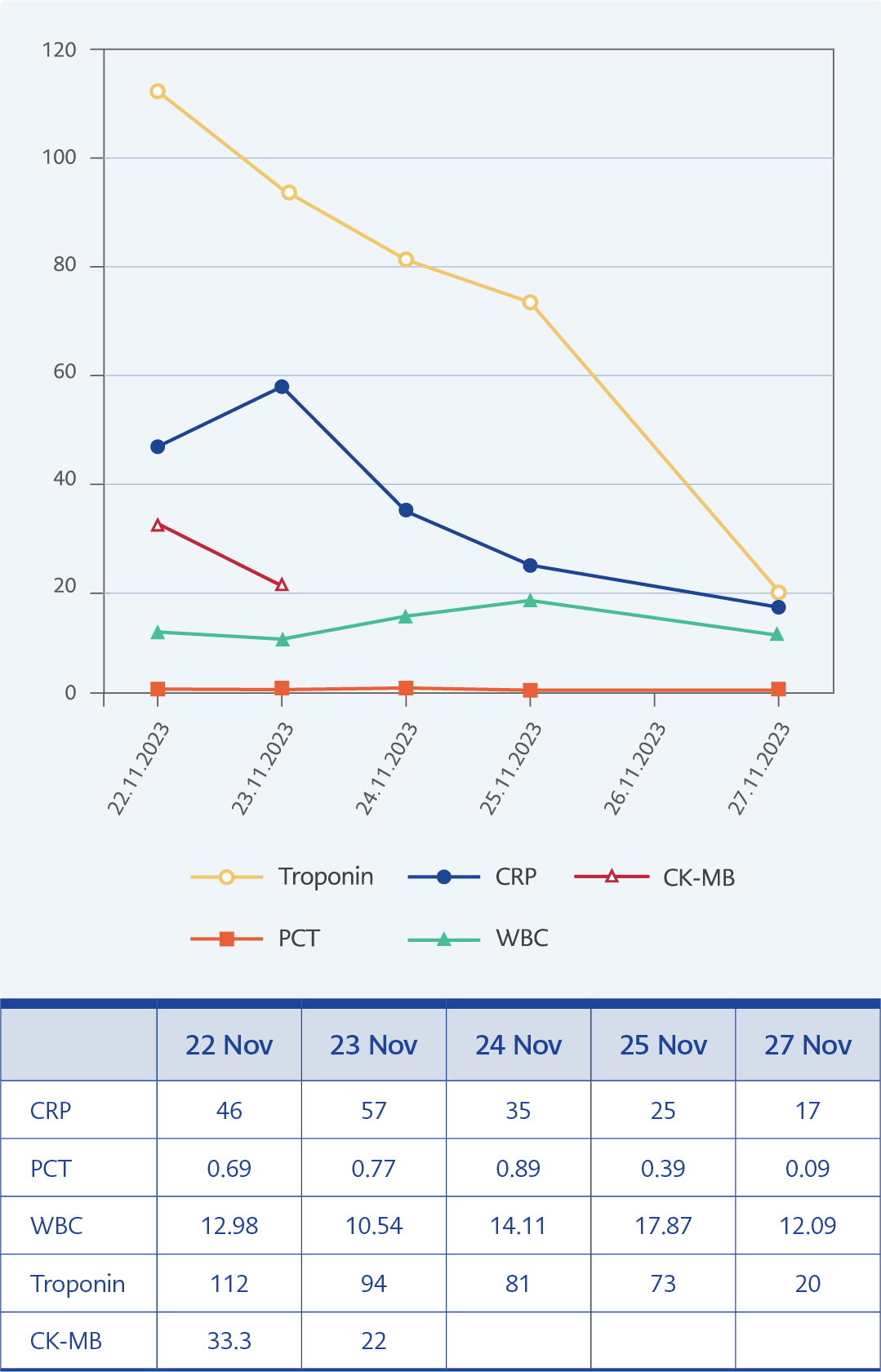
Figure 2. C-reactive protein (CRP, mg/dL), procalcitonin (PCT, ng/dL), white blood cell (WBC, K/uL), troponin T (troponin, ng/dL), creatine kinase (CK-MB, U/L).
Additionally, mild bilateral hilar lymph node enlargement was noted. The preliminary laboratory results indicated elevated levels of creatinine kinase (CK) at 997 U/L, troponin T at 112 ng/L, and acute phase reactants such as C-reactive protein (CRP) at 46.9 mg/dL and procalcitonin (PCT) at 0.69 ng/dL (Figure 2). The hemogram revealed a shift towards neutrophils, with a total white blood cell (WBC) count of 12.98 K/uL and 91% of them being neutrophils (11.8 K/uL). No bacterial growth was detected in the blood and sputum cultures. The patient was started empirical ceftriaxone intravenous 2 grams daily. The electrocardiogram (ECG) showed sinus bradycardia with a heart rate of 50 bpm and a QT interval prolongation of 520 ms. The echocardiographic evaluation revealed hypokinesia at the interventricular septum. The patient’s systematic evaluation suggested myocardial ischemia and myositis as the cause of respiratory failure. These findings indicated involvement not only in the pulmonary parenchyma but also in respiratory muscles. The etiological work-up did not reveal any underlying rheumatological, immunological, or neurological disorder, as all tests were negative, including anti-nuclear antibody, autoimmune inflammatory myopathy antibodies, anti-muscle-specific kinase antibody, anti-acetylcholine receptor antibody, and anti-voltage gated calcium channel antibodies. The patient’s history and physical examination findings were consistent with these diagnoses.
The multiplex reverse transcription PCR assay (BioFire Diagnostics, USA) conducted on the nasopharyngeal swab revealed the presence of HBoV1, leading to a diagnosis of HBoV1-induced myocardial ischemia and myositis in the patient with tested negative blood and endotracheal aspiration culture. The patient’s clinical condition improved with supportive measures, including respiratory support and intravenous methylprednisolone at a dose of 1 mg/kg. The patient was successfully weaned from invasive mechanical ventilation on the fourth day, and noninvasive mechanical ventilation was performed on the following three days. Laboratory markers such as CK and troponin T and ECG findings significantly improved. In the second week of the follow-up CT scan, the previously noted ground-glass opacities were completely resolved, with concomitant observations of atelectasis in the affected areas. This manifestation further implicated the involvement of respiratory muscles. Informed consent was obtained from the patient.
Discussion
The community-acquired HBoV1 infection in immunocompetent adult patients is rarely reported, and co-infection with other respiratory pathogens is common. In a clinical trial among immunocompetent patients, including all age groups diagnosed with respiratory tract infections, the incidence of HBoV1 was detected as 0.39%, and the co-infection rate was over 40%, mostly with Mycoplasma pneumoniae (7). In other clinical trials, low rates of positive test results for HBoV1 infection were reported in adults (8-9). The largest clinical data on adult HBoV1 infection comes from a retrospective cohort study involving 185 patients from a tertiary care center between 2010 and 2017. Of these patients, 62.2% were male with a mean age of 57 (±19), and 41.1% were immunocompromised. The most common co-pathogens in this study were rhinovirus in upper respiratory tract infection cases, adenovirus, and influenza A/B in pneumonia cases (10).
However, the case that we report is unique because she was an adult immunocompetent patient without any detectable co-pathogen and had HBoV1-induced myositis. The infection was community-acquired; probably, she acquired the infection from her four-year-old grandchild, who exhibited symptoms suggestive of an upper respiratory tract infection (URTI) a few days ago. Myositis associated with viral infections was reported before with influenza A/B, coxsackievirus, adenovirus, parainfluenza virus, Epstein-Barr virus, and cytomegalovirus (11,12), but not with HBoV1 yet. It is thought that viral myositis can be caused by either direct muscle tissue invasion or a systemic inflammatory response triggered by cytokine storm, although histopathological features are unlikely to be present (13). The diagnosis of viral myositis is based on the presence of compatible signs and symptoms, elevated muscle enzymes, suggestive electromyography (EMG) findings and muscle biopsy.
However, it is important to note that all the diagnostic tests, including the biopsy, may not yield positive, and the diagnosis may then be based on the elimination of other potential causes (11,13,14). Our diagnosis of myositis was based on physical examination findings and elevated muscle enzymes, as well as the exclusion of other potential underlying etiologies. However, the lack of an EMG examination of the patient, which may contribute to ruling out other differential diagnoses, is a potential limitation of this case report. Our case is significant because it identifies HBoV1 as a potential cause of viral myositis. At the patient’s follow-up three months later, she demonstrated no signs/symptoms or laboratory findings of myositis or myocardial ischemia.
In conclusion, HBoV1 should be considered among the differential diagnosis list of community-acquired viral pneumonia in immunocompetent adults and as a cause of myositis.