Introduction
The hazards of sandfly viruses have been known for about 100 years (1). Sandfly fever viruses of the genus Phlebovirus in the Bunyaviridae family are endemic in Mediterranean, Middle Eastern, Northern African, and Western Asian countries (2). Sandfly viruses have been reported from Italy (3), Croatia (4), Spain (5), Cyprus (6), Iran (7), and Iraq (1).
Sandfly viruses are the causative agent for a disease known as sandfly fever, phlebotomus fever or Pappataci fever. The disease was first recognized among American soldiers during World War II while they were based in North Africa. The vector of the disease (Phlebotomus papatacci), the sandfly fever Sicilian virus (SFSV) and the sandfly fever Naples virus (SFNV) were discovered by the studies of infected soldiers (8). The seroprevalence of antibodies against SFSV and SFNV is >50% in Mediterranean countries (3). In 1984, serologically confirmed clinical infections with SFSV among Swedish UN soldiers were detected in Cyprus (9).
Materials and Methods
By a retrospective chart review, the patients with fever, thrombocytopenia, and leukopenia who applied to the Başkent University Hospital in Adana between August and September 2008 and the 15 hospitalized patients with acute sandfly infection were included in the study. Acute and convalescent sera of these patients were obtained and stored at -20°C. Anti-sandfly antibodies from M and G classes were investigated with an indirect immunofluorescence antibody technique using a commercial kit (EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany). The assays were performed according to the instructions of the manufacturer. Both classes of antibodies were tested at 1:100 dilutions. The samples that were negative at 1:100 dilutions for immunoglobulin M (IgM) were retested further with the dilutions between 1:20-1:80. On the contrary, the samples positive for IgG were retested at higher dilutions ranging between1:200-1:3600. In the kit (the biochips), the substrate field was divided into four areas each of them was coated with SFSV, SFNV, Toscana virus (TOSV) or Cyprus virus (CYPV). Since these viruses are closely related both morphologically and immunogenically, cross reactions at lower dilutions might be observed, and the extension of the dilution is advised by the manufacturer for the differentiation. The samples with the highest fluorescence intensity were accepted as the responsible serotype.
Results
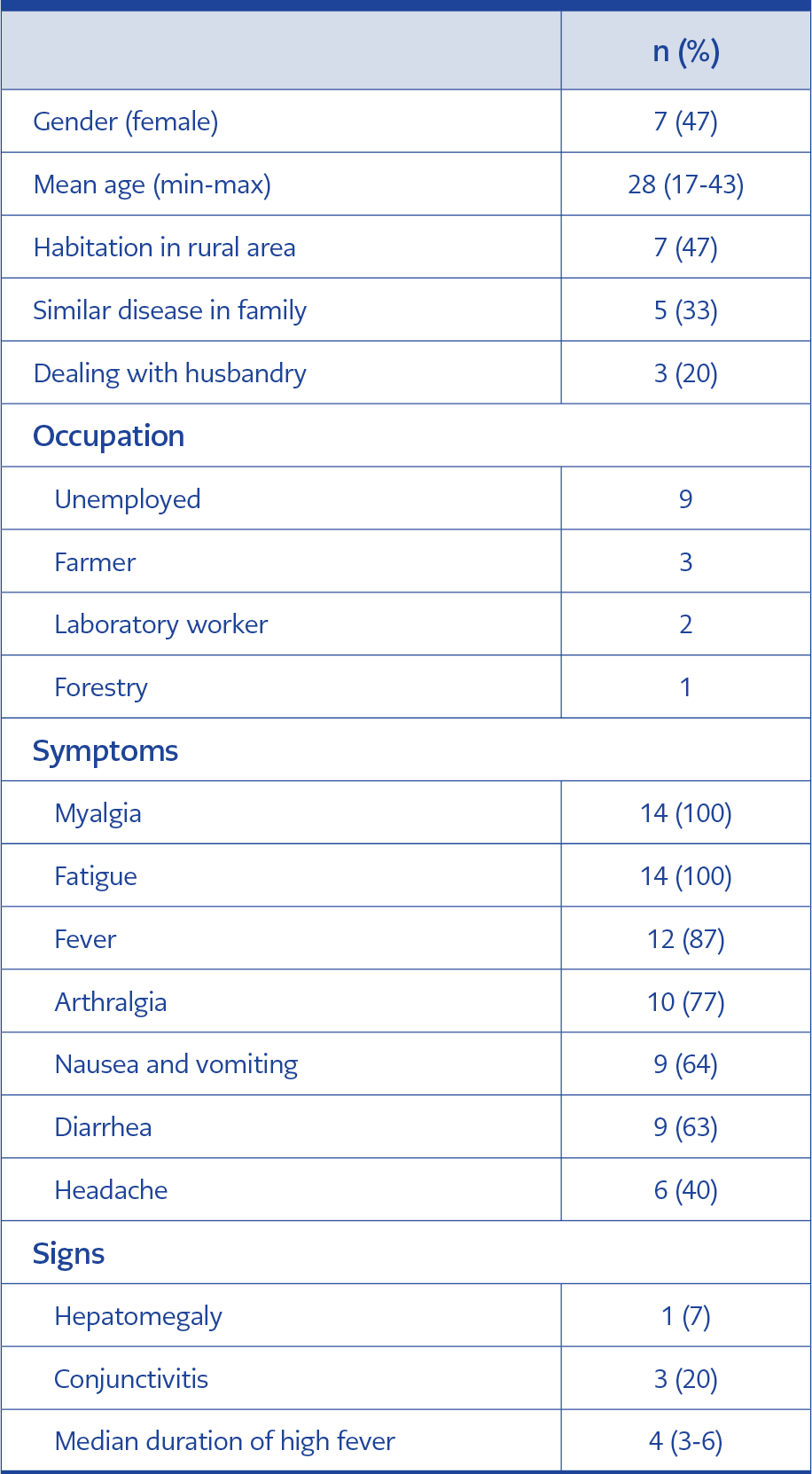
Table 1. Demographic and clinical characteristics of the patients (N=15).
The titers of IgM antibodies against Cyprus and Sicily serotypes of phleboviruses were detected to be >1/100 in 15 patients out of 21 (71%). In three patients, titers of IgM antibodies were <1/100, but the IgG levels of these patients were found to be >1/100. In 21 patients, the titers of IgG antibodies against Cyprus and Sicily serotypes were found to be >1/100. In one patient, IgM antibodies against Naples and Toscana species were found to be positive. In laboratory tests, sedimentation and chest x-ray were normal, Widal test and Wright agglutination test for Brucella, HAV, HBV, and HCV were found to be negative.
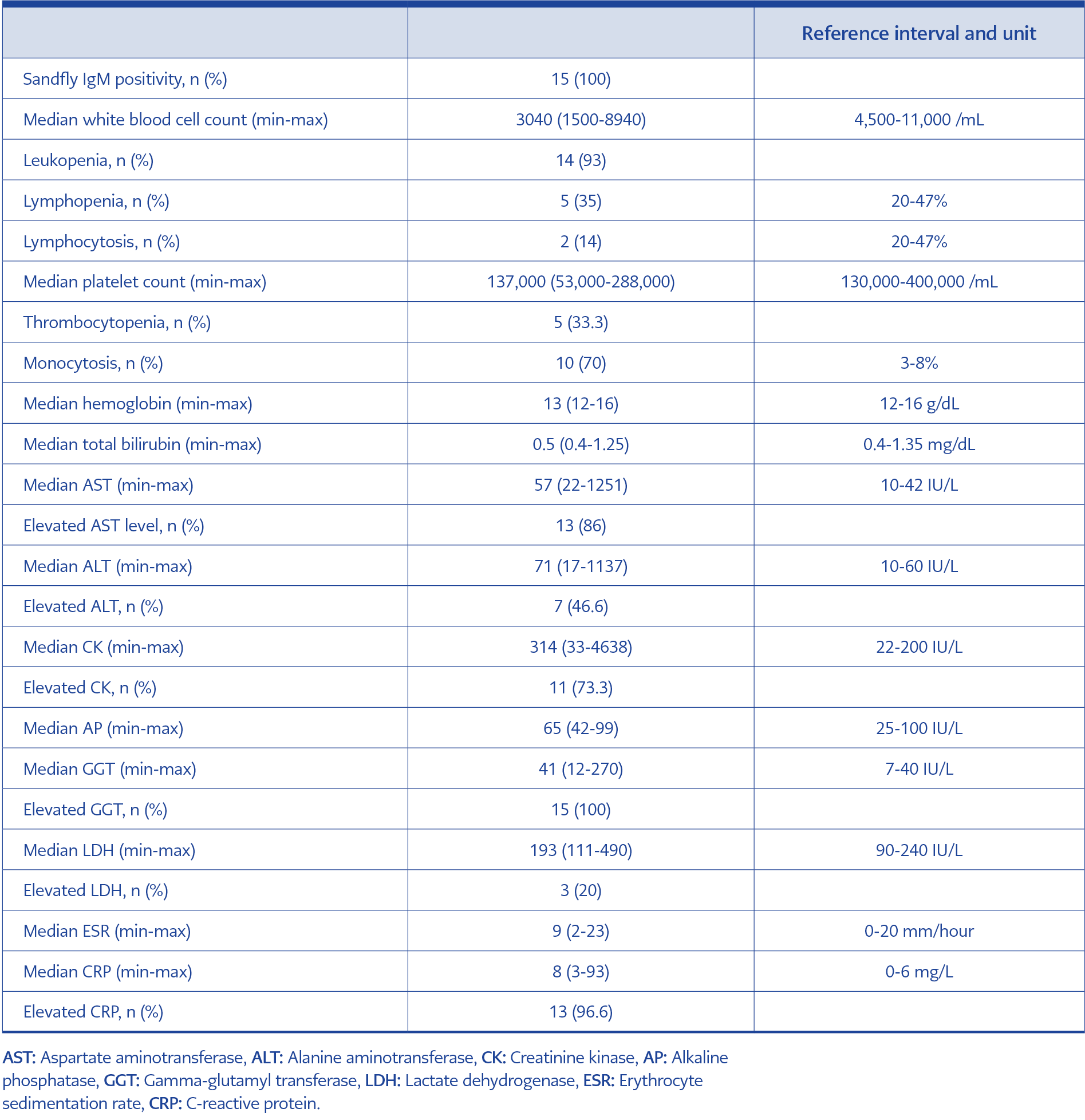
Table 2. Laboratory findings of the patients (N=15).
We presented the results of the virological confirmed 15 hospitalized patients. The mean age of the patients was 28, and 47% was female. The most common symptoms were myalgia, fatigue, fever, and arthralgia. The mean duration of the fever was four days, and the mean duration of the symptoms was 7-10 days (Table 1). The median platelet count was 137,000/mL, the median white blood cell count was 3040/mL, the median aspartate transaminase (AST) was 57 (22-1251) IU/L, the median alanine transaminase (ALT) was 71 (17-1137) IU/L, the median creatinine kinase was 314 (33-4638) IU/L, the median lactate dehydrogenase (LDH) 193 (111-490) IU/L (Table 2).
Discussion
We presented 15 confirmed and hospitalized cases infected with the sandfly virus. These were indigenous cases; 47% were from the rural regions of Adana, with a mean age of 28 years and almost equal gender distribution (Table 1). In 1/3 of the patients, there were infected cases in the family. The characteristics of 40 patients with similar clinical and laboratory features were presented in 2001. These cases were attributed to arboviruses but not specifically to the sandfly viruses (10). In the summer months of 1998, following an earthquake in Adana, hundreds of patients with similar symptoms, signs, and laboratory findings were described (observations of Önder Ergönül while he was working in Adana Numune Hospital as an IDCM specialist). In this case series, the most common symptoms and signs were myalgia, fatigue, fever, headache, arthralgia, conjunctivitis, nausea, and vomiting (Table 1). Fever was >39°C and responded to nonsteroidal anti-inflammatory drugs. In laboratory analysis, the median white blood cell and thrombocyte counts were lower, and AST and ALT were elevated (Table 2). In the follow-up of the patients, the total duration of the fever was 72 hours, and the fever stopped abruptly. Fatigue, myalgia, and back pain lasted approximately seven days. There was no skin rash, lymphadenopathy, meningeal irritation, or recurrence.
The clinical characteristics of the patients should be differentiated from those of other infectious diseases in the region, such as Crimean-Congo hemorrhagic fever (CCHF). CCHF infection was not reported from Adana but should be considered in different parts of Türkiye. Leucopenia, thrombocytopenia, and elevation of liver enzymes are common features among viral infections. Sandfly infections are milder and self-limited than CCHF infections (11).
According to the clinicians in the region, the number of cases decreased over the years. In 2001 and 2002, there were 5-6 patients each week in the summer months. The cases were reported between April and September and, more commonly, in the province of Adana, located in the Mediterranean Region of Türkiye. In this region, the summer months are very hot and humid. Both the CCHF virus and phleboviruses are members of Bunyaviridae. The occurrence of these viruses could be associated with climate change and also after natural disasters (12).
The season for the sandfly infection is from April to October. However, we were able to collect samples in August and September because of the delayed detection of the infection. The retrospective character of our study design did not allow us to collect data for additional cases. It was likely that there were a higher number of cases that we could not diagnose and detect. Sandfly fever seems to be endemic in the Southern part of TÜrkiye, where cases occur sporadically or in outbreaks.
In serotyping, the antibody response of almost all patients against Cyprus/Sicily strains is consistent with the epidemiological data of our region. On the other hand, Naples/Toscana positivity in one patient can be explained by a cross-reaction due to the close immunogenetic properties of the strains.
In conclusion, clinicians should consider sandfly fever in the differential diagnosis of patients with symptoms like those described above, particularly if the patient has recently visited an endemic region. Monitoring the viral RNA in midges will help determine the likelihood of infection and outbreaks. However, measures for the prevention of the disease (e.g., protective clothing and use of insect repellent) should be taken in endemic areas, especially during the summer, when sandflies are active.