Introduction
A 78-year-old male patient with diagnoses of diabetes, hypertension, and gout presented with fever, night sweats, weight loss, and back pain for the past two months. On physical examination, he had a body temperature of 37.5°C and tenderness on palpation in the thoracolumbar region. His white blood cell (WBC) count was 14,680/uL, C-reactive protein (CRP) 178 mg/L, and erythrocyte sedimentation rate (ESR) 76 mm/h. Blood and urine cultures were negative. Rose-Bengal, the Wright agglutination test, and Brucella IgM and IgG were negative. Contrast-enhanced magnetic resonance imaging (MRI) revealed an abscess-like area extending into the anterior paravertebral space. He declined biopsy and lumbar puncture procedures. We started ceftriaxone 2×1 and vancomycin 2×1 intravenous (IV) as empirical treatment. He had a family history of tuberculosis (TB) and had lived in an endemic area for a long time. His QuantiFERON test was positive. There was no significant change in symptoms and inflammatory markers during the first month of empiric treatment. The patient’s control thoracolumbar MRI is shown in Figure 1. Anti-TB treatment was initiated. The patient’s symptoms were relieved, and inflammatory markers decreased after one month of treatment. We discharged him with the prescribed anti-TB therapy and evaluated him at follow-ups in the third, eighth, and 12th months. In the 12th month follow-up, WBC was 5760/uL, CRP 14 mg/L, ESR 53 mm/h and showed regression on the MRI (Figure 2).
Tuberculous spinal infections should be suspected in patients with an insidious, progressive history of back pain and individuals from an endemic area. The clinical, hematologic, and radiologic parameters can be used to declare a spinal tubercular lesion healing (1)

Figure 1. Sagittal T1 weighted image without fat suppression (A); Abscess formation (asterisk) extending into the anterior paravertebral space and sagittal T1-weighted fat-suppressed contrast-enhanced images (B, C); Contrast increases were observed around the abscess, in the intervertebral disc space and in the vertebral end plates (arrows).
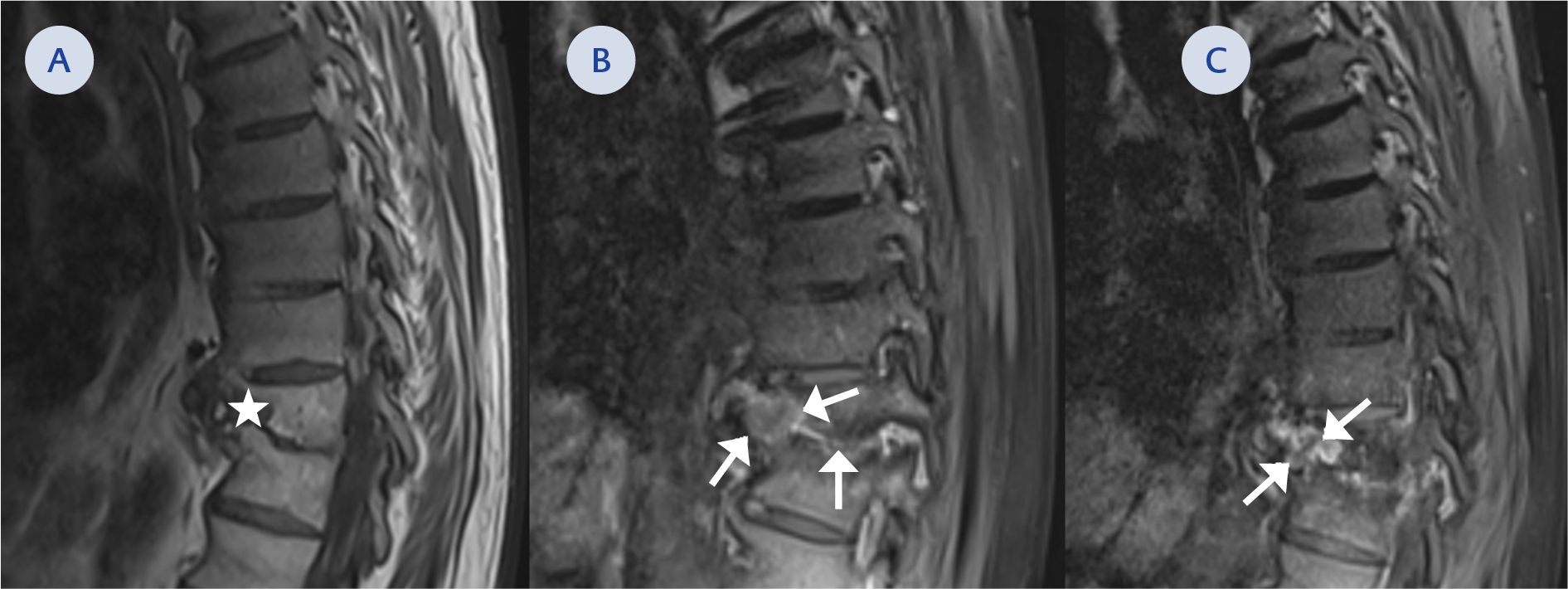
Figure 2. Sagittal T1 weighted image without fat suppression (A); Decrease in size of abscess formation (asterisk) and sagittal T1-weighted fat-suppressed contrast-enhanced images (B, C); A regression of contrast enhancement was observed around the abscess, in the intervertebral disc space and in the vertebral end plates (arrows)