Introduction
Pyomyositis is a primary infection of skeletal muscle that does not result from a contiguous disease, is hematogenous in origin, and often results in abscess formation. Although pyomyositis is classically an infection in tropical regions, it is an emerging infection in temperate climates. Pyomyositis is frequently caused by aerobic Gram-positive and Gram-negative bacteria (1). Staphylococcus aureus (~90% in tropical regions and 75% in temperate regions) is the most commonly isolated bacterium. Pyomyositis caused by Mycobacterium tuberculosis is extremely rare. Here, we report a patient with tuberculous (TB) pyomyositis.
Case

Figure 1. Macroscopic appearance of the swelling.
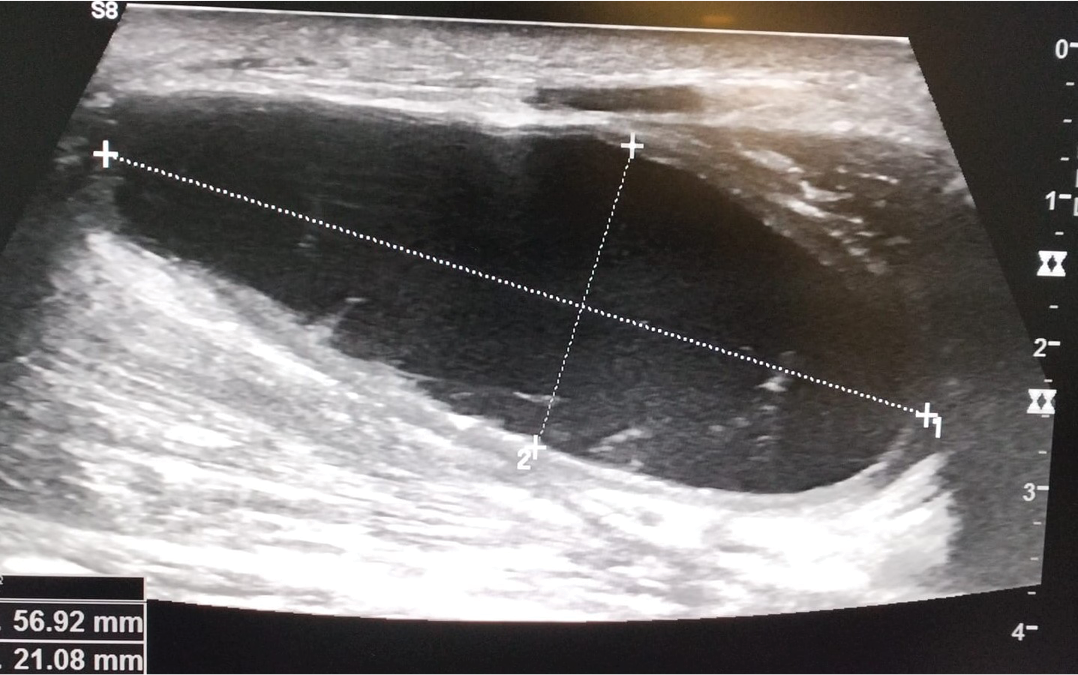
Figure 2. Ultrasound examination showing pus collection in the muscle.
A 51-year-old male patient applied with a year history of painless, progressively increasing swelling volar face of the left forearm. There was no history of fever, weight loss, anorexia, trauma, diabetes, immunosuppression, corticosteroid use, and renal failure. His history was negative for recent TB or contact. Physical examination showed significant swelling of the left forearm without erythema, tenderness, or warmth to palpation (Figure 1). There were two BCG scars, and QuantiFERON®-TB Gold Plus was 2.67 IU/mL (0 – 0.35 IU/mL). All laboratory tests, such as C-reactive protein (CRP), erythrocyte sedimentation rate, biochemistry and hemogram, were within normal limits. Radiographs of the chest revealed no evidence of pulmonary TB. The HIV antibody test was negative. Ultrasonography revealed a thick-walled, dense collection approximately 100 mm in length and 21 mm in depth between the muscle planes on the volar face of the left forearm (Figure 2).
The intramuscular abscess containing a large amount of fibrinous pus collection was drained and was positive for acid-fast bacilli (AFB) by Ehrlich-Ziehl-Neelsen (EZN) staining. The sample was positive for M. tuberculosis complex DNA, which was tested using the GeneXpert® MTB/RIF Ultra system (Cepheid, USA). M. tuberculosis complex was grown from pus two weeks later using the BD BACTEC™ MGIT™ automated mycobacterial detection system (liquid media) (Becton Dickinson, USA). Histopathology of muscle showed CD68+ cells (histiocytes) around necrosis, chronic inflammation and granulomatous reaction consistent with TB pyomyositis. AFB was not seen on EZN staining of the granulomatous tissue. The diagnosis of TB pyomyositis was made, and the patient was successfully treated with the traditional regimen (intensive phase: 2 months and maintenance phase: 4 months), including the drugs isoniazid, rifampin, pyrazinamide and ethambutol.
Discussion
TB remains a major public problem. Musculoskeletal TB occurs in ~10% of patients with extrapulmonary tuberculosis (2), while TB pyomyositis is extremely rare. Case reports of TB pyomyositis are very limited in the literature but are gradually increasing due to the widespread use of immunosuppressive drugs and the HIV/AIDS pandemic. In daily practice, M. tuberculosis is not considered in the etiology of primary muscle abscesses. Pyogenic pyomyositis and TB pyomyositis cannot be distinguished on the basis of clinical and radiological findings.
Most TB pyomyositis cases reported in the literature were treated empirically with antibiotics following a preliminary diagnosis of pyogenic pyomyositis (3-14). Radiographic imaging, such as ultrasonography, computed tomography, and magnetic resonance imaging (MRI), are the most helpful tools in the diagnosis of pyomyositis. MRI is the optimal imaging technique and is highly sensitive to muscle inflammation, even before the formation of a frank abscess. The definitive etiological diagnosis of pyomyositis is made by microbiological and pathological examination of the appropriate sample (pus or tissue). It is made by the isolation of M. tuberculosis in the pus or tissue sample or by histopathological evidence of TB in any relevant tissue sample. Gram and EZN staining of pus, as well as TB-PCR study results, are available within two hours. The bacteriological diagnosis of pyomyositis is traditionally made from cultures of surgical specimens. Pus or tissue culture using a Lowenstein-Jensen medium and mycobacteria growth indicator tube (MGIT) detection system is the gold standard for TB diagnosis.
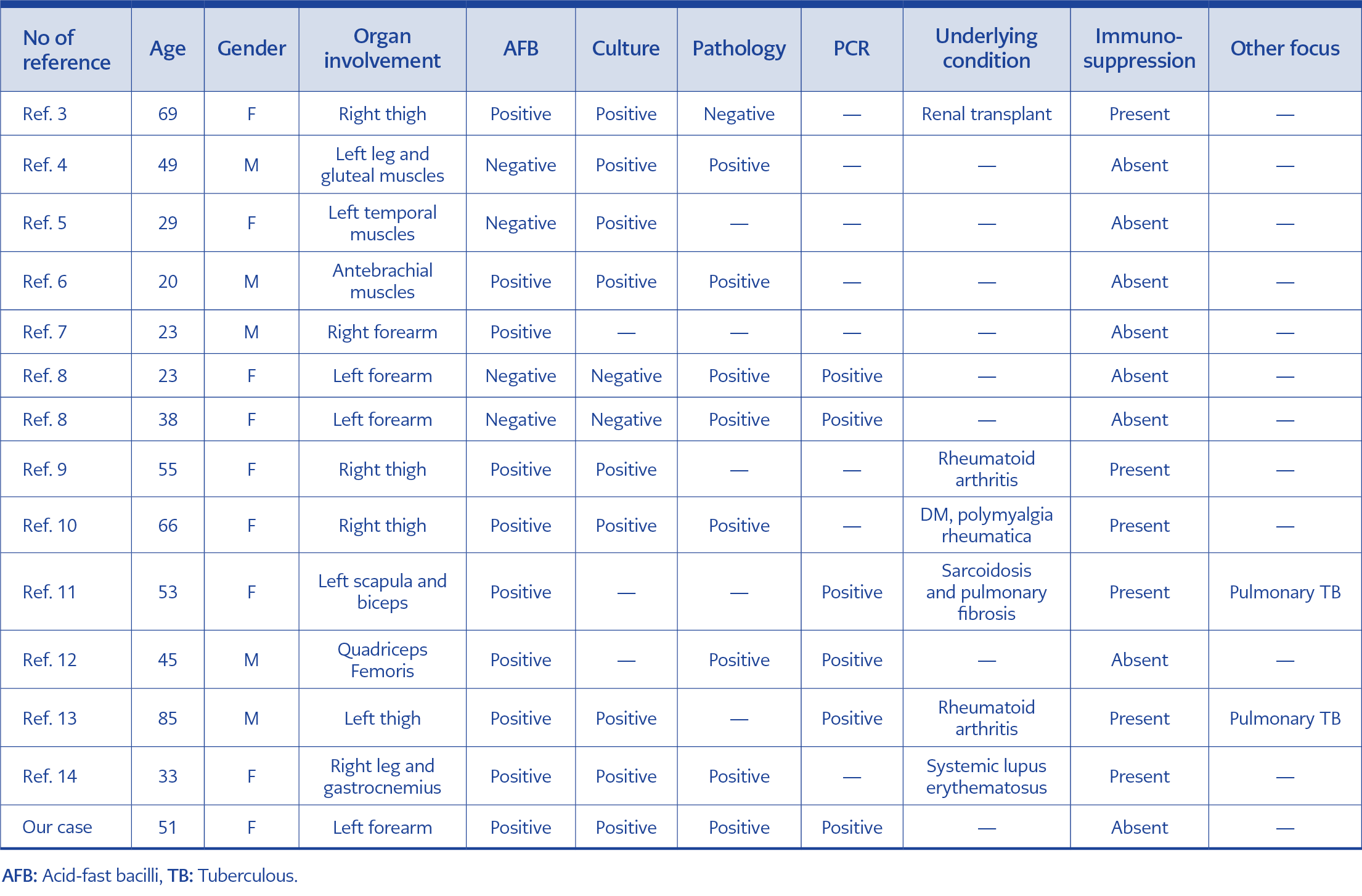
Table 1. Main characteristics of the cases.
AFB, PCR, and culture positivity rates were 92%, 100%, and 82%, respectively, in 13 cases with TB pyomyositis that we reviewed from the literature (3-14). The characteristics of all patients, including our report, are shown in Table 1. Although no TB focus was detected in our case, pulmonary TB had been diagnosed by TB culture and PCR in two patients. In addition, immunosuppression was present in almost half of the patients. In our case, all tests, including AFB, PCR, culture and histopathology, were performed and were all positive. Smear microscopy by EZN to detect AFB remains the mainstay of TB diagnosis. However, it is difficult to detect less than 10,000 bacilli per mL with this method (15).
In conclusion, in all cases of TB pyomyositis with abscess, M. tuberculosis should be investigated in addition to Gram staining and aerobic culture on the first pus sample. Thus, the diagnosis can be made without delay, resulting in good functional recovery with adequate drainage and anti-TB treatment.