Introduction
Human immunodeficiency virus (HIV) remains a significant global health challenge with societal impacts. Despite a decline in the annual number of new cases worldwide, the incidence of HIV is on the rise in the Eastern Europe/Central Asia region, including Türkiye (1). With the introduction of new antiretroviral treatments (ARTs), HIV has transitioned from a progressive disease to a chronic, stable, and manageable condition (2). Despite substantial advancements in treatment, patients continue to experience physical and psychological challenges due to social issues, lifelong treatment regimens, and treatment side effects. In addition to the physiological effects on patients, HIV infection also represents a source of chronic stress with social and societal dimensions (3). Prejudices towards people living with HIV (PLWH), compounded by misinformation about transmission routes, contribute to discrimination and stigmatization in Türkiye and globally (4, 5). Societal stigmas, loss of social support, and fear of abandonment create fertile ground for psychological issues. Previous studies have identified anxiety and depression as the most prevalent mental disorders among PLWH (6, 7). Therefore, behavioral, psychosocial, and holistic interventions have become essential to mitigate the effects of the disease, complementing existing treatments (2, 7).
The time required for hospital visits, treatment costs, concerns about confidentiality, and stigmatization can act as barriers to accessing traditional in-person care, posing significant challenges for PLWH (8, 9). Telerehabilitation, an emerging platform, offers a solution to reach and accommodate patients who may be unable to attend clinic appointments in person. By providing an online environment where patients cannot see each other, telerehabilitation allows participants to engage anonymously, offering a promising alternative to traditional in-person sessions.
Starting from the premise that individuals are psychosocial entities and recognizing the importance of a holistic treatment approach, the Cognitive Exercise Therapy Approach (BETY) has been implemented in various chronic diseases (10, 11). BETY is an innovative approach that aims to shift the patient’s negative thoughts related to the disease into positive ones during exercises and promote the development of positive thoughts through engaging activities like drama (12).
In this study, we aimed to investigate the efficacy of BETY delivered through telerehabilitation among adults living with HIV and to demonstrate the evidence-based feasibility of this approach.
Materials and Methods
The study included virologically suppressed PLWH receiving ART and undergoing follow-up at the Infectious Diseases and Clinical Microbiology Polyclinic of Şanlıurfa Training and Research Hospital between May 2022 and May 2023.
Of the 50 PLWH who agreed to participate and met the inclusion criteria, 25 were willing to engage in telerehabilitation and possessed the cognitive capacity to follow video conferences, forming the telerehabilitation group (TG). The remaining 25 formed the control group (CG). The preliminary results presented include data from 10 patients in TG and 15 patients in the CG who completed the 12-week treatment.
The TG patients were divided into three groups based on their availability for sessions: morning, afternoon, and evening. Three distinct physiotherapists conducted these sessions. Each of these physiotherapists had undergone 60 hours of BETY training before the study and possessed at least five years of clinical experience.
All protocols adhered to the ethical guidelines outlined in the Declaration of Helsinki. The Non-Interventional Research Ethics Committee of Hasan Kalyoncu University approved the study on March 18, 2022 with decision number 2022-024. Written informed consent was obtained from all the participants. This study was registered in the WHO International Clinical Trials Registry Platform (NCT05342337).
Measures
Before initiating the study, comprehensive records were compiled for each patient, encompassing physical characteristics, sociodemographic information (including age, gender, height, weight, education level, probable route of infection), and exercise habits. Body mass index (BMI) was calculated by dividing body weight by the square of height (kg/m2).
The biopsychosocial status of the patients was assessed using the Cognitive Exercise Therapy Approach-Biopsychosocial Questionnaire (BETY-BQ). The BETY-BQ is a scale developed based on patient feedback and specialist opinions to address the limitations of existing questionnaires used for years in patients with chronic rheumatismal diseases treated with the BETY principles. The BETY-BQ comprises 30 items that provide insights into pain, socialization, mood, sexuality, functionality, and sleep quality. Each item in the scale is scored from 0 to 4 points using Likert-type responses (4: yes, always; 3: yes, usually; 2: yes, sometimes; 1: yes occasionally; 0: no, never). Higher points indicate a poorer biopsychosocial status (13).
The patient’s quality of life was assessed using the Short Form-36 (SF-36). This questionnaire includes eight subscales: physical function, social function, role limitations related to physical problems, pain, vitality, mental health, and general health perception. Each subscale is scored on a scale of 0 to 100 points, with scores not being totalled. A higher score indicates a better health status (14).
Participants were evaluated using the Hospital Anxiety and Depression Scale (HADS), the Clinical Fragility Scale, and the FRAIL Scale. The HADS consists of 14 items, each featuring four response options that refer to the recent past. Odd-numbered items assess anxiety, while even-numbered items assess depression. Separate scores are derived for anxiety and depression (15). The Clinical Fragility Scale is a subjective assessment of fragility, offering preliminary insight into the risk of care home admission and mortality. Following clinical evaluation, the clinical fragility score is determined by assigning a score from 1 (very active) to 9 (terminal disease) (16). The FRAIL scale consists of five items, enabling evaluation through inquiries about the patient’s fatigue, resistance, mobility, weight loss, and other diseases. Patient responses are scored as 0 or 1 point, and the total score is classified as 0: resistant (non-frail), 1-2: pre-frail, and >2: frail (17).
The BETY Protocol
In addition to the standard treatments, the TG patients engaged in group rehabilitation exercises based on the BETY principle (12), supervised by a physiotherapist via a video conference platform. These sessions lasted for 60 minutes, three days a week, over 12 weeks (totalling 36 sessions). Before commencing group exercises, the BETY method was introduced, and patients were educated on proper neck, shoulder, rib cage, and lumbopelvic positioning, and correct breathing techniques during the initial session. Subsequent sessions involved telerehabilitation-based treatment, where each patient accessed the Zoom platform using a chosen username. To ensure privacy, sound and video feeds of other patients were disabled, preventing them from seeing or hearing each other. Each one-hour session comprised warm-up exercises, the exercise routine, and a cool-down phase. A physiotherapist demonstrated exercises and provided guidance through videos.
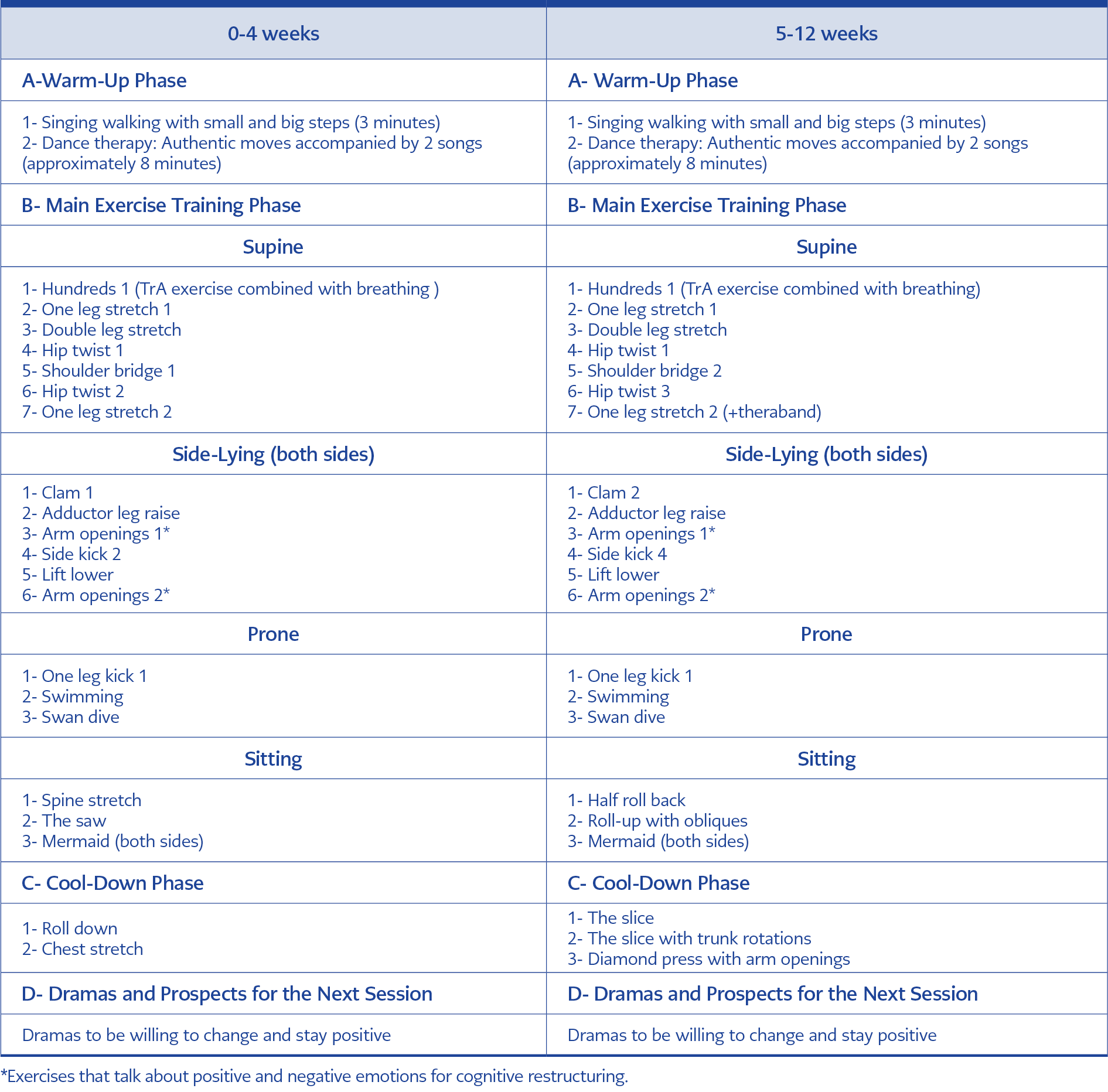
Table 1. The cognitive exercise therapy approach (BETY).
During the warm-up and cool-down periods, dance therapy involving authentic movements to music was employed. In the exercise phase, functional trunk stabilization exercises were performed (Table 1). Exercise intensity was progressively increased using resistance bands based on each patient’s progress to align with the loading principle. The CG continued with their regular drug treatments without any supplementary interventions. After the 12-week treatment period, the responses to the scales were compared between the two groups.
Statistical Analysis
The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 23.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov test was performed to assess the normality of the samples’ distribution. The Wilcoxon Test was used to compare the pre- and post-treatment values within each group. The statistical significance was set as p<0.05.
Results
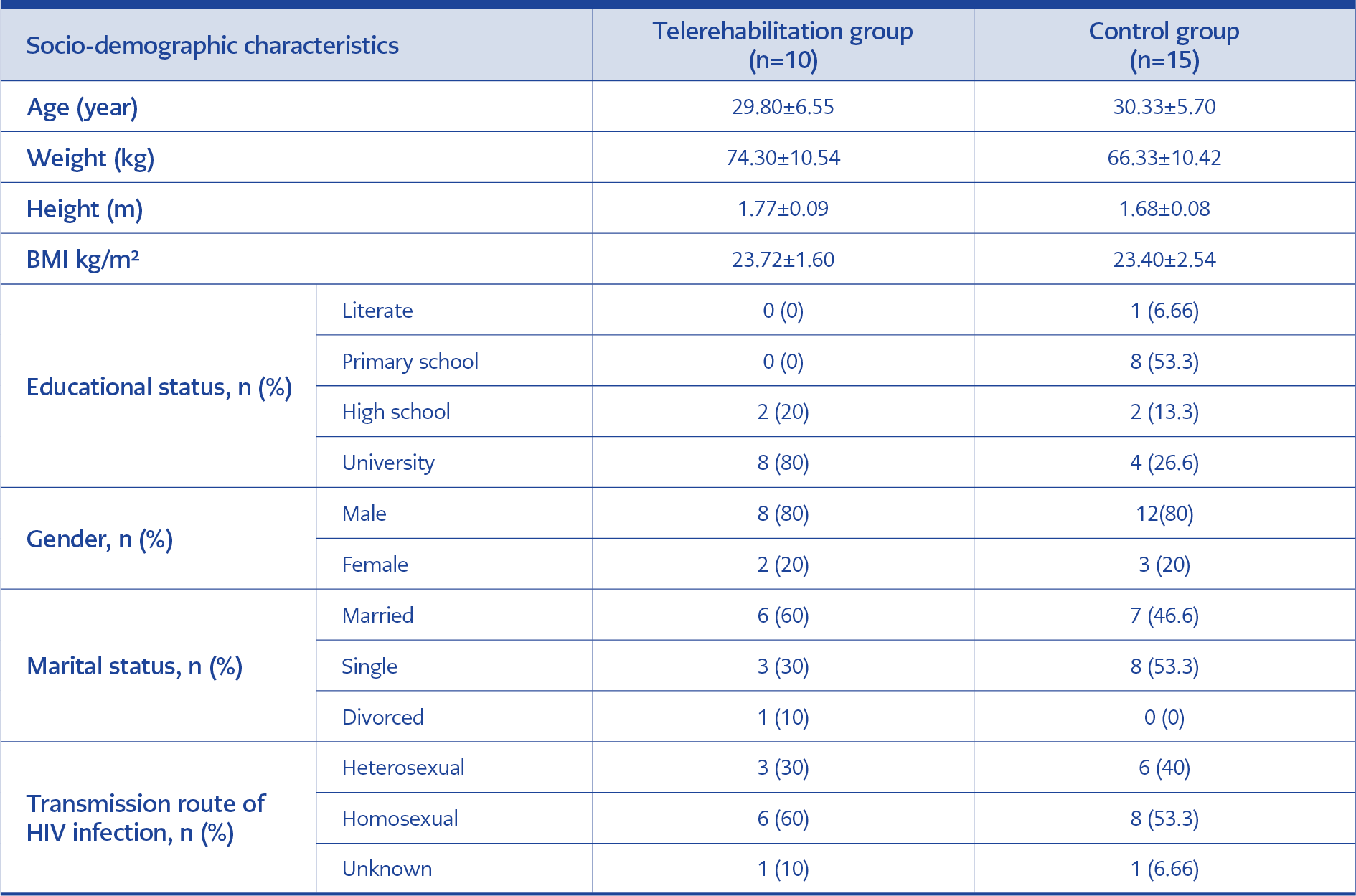
Table 2. Socio-demographic characteristics of the participants.
The study initially included 25 TG and 25 CG patients. The sociodemographic characteristics of the 10 TG patients who completed the exercise treatment and 15 CG patients are presented in Table 2. Among the TG, there were eight males and two females, with a mean age of 29.80 years (range 23-45 years). In the CG, there were 12 males and three females, with a mean age of 30.33 years (range 22-42 years). Age, gender, and BMI were similar, with a greater number of males in both groups (p>0.05).
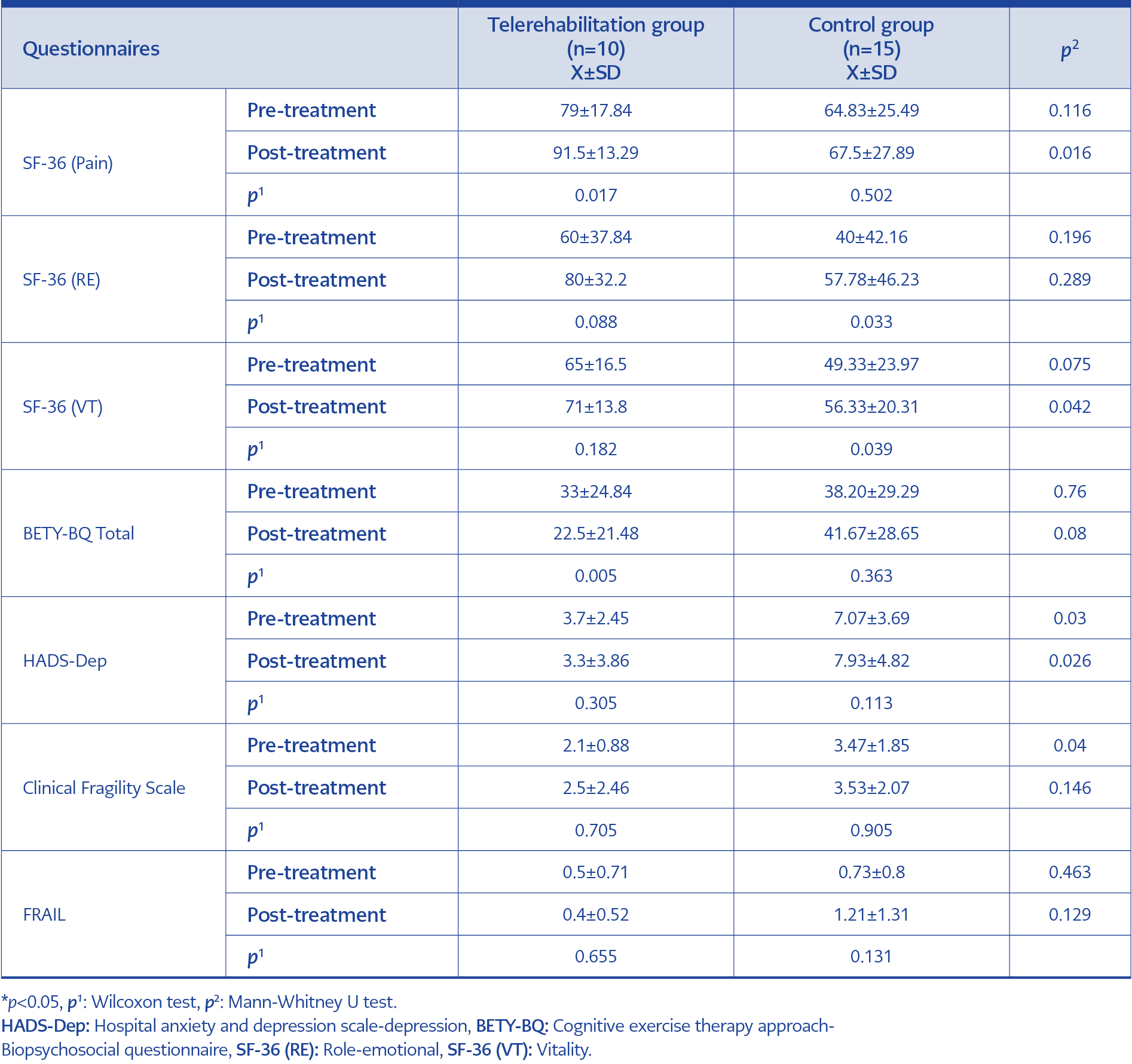
Table 3. Pre- and post-treatment scale evaluation results of telerehabilitation group and control group.
The results of the scale evaluations of the TG and CG are shown in Table 3. A greater improvement was determined in the SF-36 pain sub-parameter and the BETY-BQ total score in the TG (p=0.017), while the difference between the groups was found to be statistically significant (p=0.016). The SF-36 pain score increased from 79 to 91.5, indicating an improved quality of life. The BETY-BQ total score decreased from a mean of 33.0 to 22.50, signifying a significant enhancement in biopsychosocial status in the TG after treatment (p=0.005). In the CG, a statistically significant difference was identified in the SF-36 sub-parameters of emotional role difficulty (p=0.033) and vitality (p=0.039).
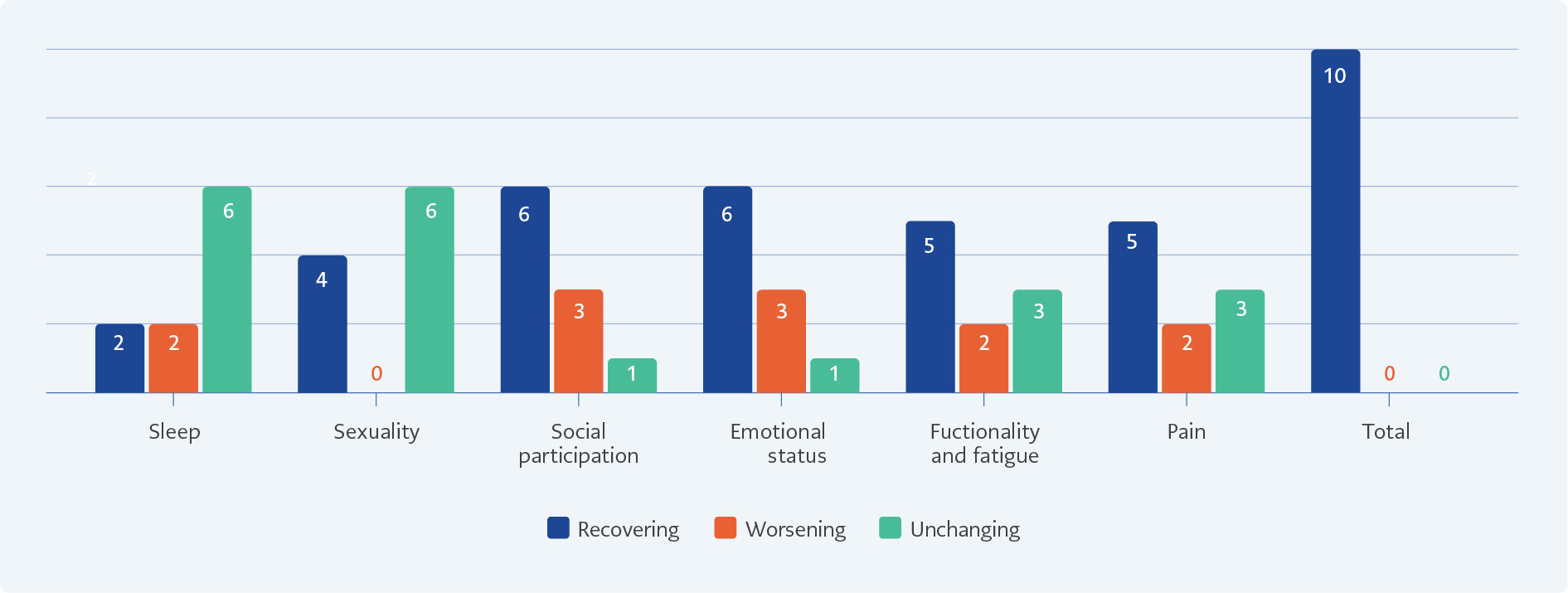
Figure 1. BETY-BQ data of telerehabilitation group.
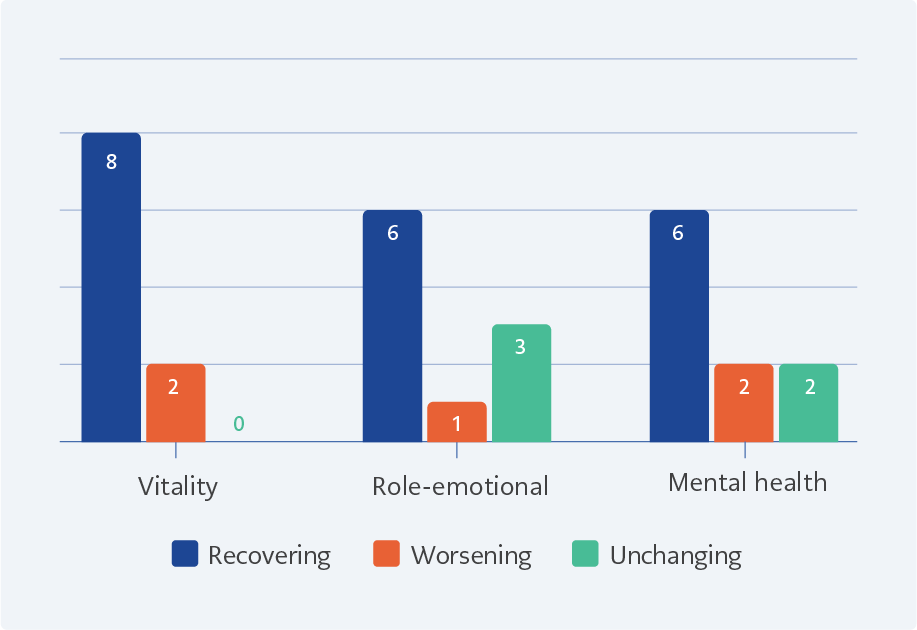
Figure 2. SF-36 data of telerehabilitation group.
In this study, which presented preliminary results, the evaluation of BETY-BQ parameters within the TG revealed statistically significant differences only in the total score due to the limited number of patients (p=0.005). Detailed examination of the outcomes showed enhancement in sub-parameters in most patients and improvements in the total BETY score for all patients (Figure 1). There were no statistically significant differences in the individual results of the SF-36 sub-parameters for vitality, emotional role difficulty, and mental health after treatment. However, clinical improvement was determined in most of the TG patients (Figure 2).
The feedback provided by the patients after the study revealed significant improvements in their psychological well-being, increased vitality, and enhanced self-confidence. These patient testimonials highlight the positive impact of the study’s intervention on their well-being and offer valuable insight into their experience. Some examples of the feedback from the patients are given below:
User Name- Özay: “I now experience much less fatigue, and cognitive exercises have significantly reduced my negative feelings. While concerns about the future remain, they are now more manageable. I have established a consistent exercise routine.”
User Name- Manolya: “Upon joining this group, I realised I lacked proper breathing techniques. My pain has diminished to the point of being nearly negligible. I commence each day with heightened energy levels, and my psychological state has notably improved.”
User Name- Ruhum: “Previously, I faced significant distress when visiting the hospital due to societal prejudices and opinions. Now, I am at ease, fully aware of my worth. I find greater comfort and diminished fatigue.”
Discussion
In this study, we investigated the efficacy of the BETY program, which was applied through telerehabilitation, among PLWH. The findings indicated that the 12-week BETY program significantly reduced pain and enhanced participants’ biopsychosocial status.
Effective ARTs have substantially decreased the morbidity and mortality rates associated with HIV infection, marking a significant advancement in global public health. However, patients still encounter various comorbidities that can compromise their health outcomes. The management of these comorbidities within the framework of HIV, now recognized as a chronic infectious disease, requires a multifaceted approach that addresses not only the viral infection but also the associated health challenges. Comprehensive, holistic, and psychosocial interventions are essential to this management strategy.
A 2019 study gathering perspectives from healthcare workers and PLWH on integrating HIV care with physiotherapy professions found that including physical therapy within a multidisciplinary treatment approach is beneficial (18). A meta-analysis investigated the effects of aerobic exercise on immunological, viral, cardiorespiratory, strength, body composition, and psychological well-being among PLWH. It revealed that medically stable individuals who participated in aerobic or combined aerobic/resistance exercises experienced notable improvements in cardiorespiratory function, quality of life, and psychological well-being (19). Our current study supports these findings, with participants reporting increased health, energy, and self-confidence after a 12-week treatment program. Although many had initially avoided exercise due to fatigue and lack of motivation, their views on physiotherapy became overwhelmingly positive throughout the course of treatment, underscoring its significant impact on their overall well-being.
The rising necessity for telerehabilitation among PLWH can be attributed to the social stigma they face, their preference for privacy during exercises, and the logistical challenges of hospital visits (20). Bonato et al. conducted a study facilitated by a smartphone app and reported improvements in cholesterol levels, posture, psychological well-being, and cardiovascular vitality (21). In this study, a clinician supervised the participants using the mobile application during the first four weeks, after which patients continued the exercises independently for the next 12 weeks. Interestingly, participation rates were notably higher when patients were supervised by a clinician, highlighting the potential benefits of individualized follow-up.
The first randomized controlled trial focusing on telerehabilitation for HIV infection was conducted in 2019 by Piraux et al., with no significant differences noted between the two exercise groups. However, the study highlighted the need for further exploration of telerehabilitation methods (2). Pain is a frequently observed symptom among PLWH, presenting in various forms in up to 90% of cases across all stages of the disease (22). da Silva et al. investigated the correlation between the quality of life and pain levels in PLWH and revealed that 65% of patients experienced severe pain that significantly worsened their health status. Their findings also noted a strong association between pain complaints and various aspects of quality of life, including psychological well-being, independence and social relationships. Moreover, factors such as societal acceptance, body image, self-confidence, and positive emotions were found to be impacted by pain severity (23).
In the quality-of-life assessment within the present study’s telerehabilitation group, a significant improvement was observed in the SF-36 pain parameter, characterized by an increase in the mean score from 79 before treatment to 91.5 post-treatment. Patients reported not only reduced pain levels but also diminished daytime fatigue. This reduction in pain could be attributed to several factors: the emphasis on trunk stabilization exercises, the focus on maintaining respiratory control during exercises, and the integration of proper breathing techniques into daily activities. The structured treatment approach was also designed to prevent stigmatization alongside the establishment of trustworthy relationships with healthcare professionals who provided consistent support under all circumstances. Moreover, the cognitive engagement fostered by the BETY approach likely enhanced psychological comfort, further contributing to the overall reduction in pain.
Depression and anxiety are the most prevalent mental health disorders and pose significant challenges for PLWH, reducing overall quality of life and potentially diminishing the efficacy of ART (24). An investigation highlighted that engaging in recreational exercise led to improved quality of life by alleviating anxiety and depression within a German population of PLWH (6). In the present study, mental health was assessed using the HADS. While the overall improvement in the TG was not statistically significant, a detailed analysis of individual results revealed that seven out of the ten patients showed enhancements in their total HADS scores. The absence of a statistically significant result across the group could be attributed to the small sample size.
Upon reviewing the existing literature, no studies were found that investigated biopsychosocial interventions and evaluations specifically targeting PLWH. Notably, in the current study, the most remarkable improvement was observed in the BETY-BQ total score of the TG. This study’s noteworthy strength lies in its emphasis on a biopsychosocial approach. The findings suggest that incorporating elements like dance therapy with authentic movements set to music at the outset of each session, alongside cognitive restructuring during exercise, proves efficacious in both physiological and psychological domains. Furthermore, the group sessions foster social improvement.
Rehabilitation aims to establish consistent exercise routines and develop an exercise habit while addressing a variety of chronic conditions, including HIV infection. BETY provides a platform for patients to improve their exercise habits by incorporating a biopsychosocial dimension that transforms negative cognitions into positive ones through dramatic engagement. Advances in medical treatments have extended the lifespan of PLWH. BETY stands out as an innovative alternative in this field among holistic approaches aimed at enhancing the quality of life for PLWH, preventing comorbidities, and emphasizing the necessity of biopsychosocial support in today’s world.
This study, presenting preliminary results, has certain limitations. The sample size was relatively small, and randomization could not be executed due to the insufficient number of patients with active internet utilization, potentially impacting the outcomes. Additionally, the absence of comparable studies in the existing literature implementing biopsychosocial interventions in PLWH makes result comparisons unfeasible.
Based on the preliminary findings of this ongoing study, it is evident that the application of the BETY method through telerehabilitation effectively reduces pain and improves the biopsychosocial status of PLWH. Cognitive exercise therapy BETY, delivered by telerehabilitation, shows promise as a viable treatment modality for PLWH. Further research and validation are warranted to confirm these promising results.